INI-CET 2017 — Pathology
5 Previous Year Questions with Answers & Explanations
The following brain biopsy of patient who presented with marked psychomotor agitation is diagnostic of?
A 70-year-old man presents with history of intractable diarrhea. His bone marrow and kidney biopsy are shown below. Which of the following is the most appropriate diagnosis?
A 35-year-old presented with fever. On examination he had enlarged and ulcerated tonsils. Since peripheral smear shows lymphocytosis, monospot test was done which is negative. Tonsillectomy was done and stained section is shown below. Large cells mixed with lymphocytes are seen. The cells are positive for CD20, EBVLMP-1, MUM1, CD 79a and CD 15 negative. The background cells are positive for CD3. Diagnosis is: (AIIMS May 2017)
The following is a picture from scrapping of genital ulcer. Comment on the diagnosis. (AIIMS May 2017)
The vacutainer shown below is used for collecting sample for? (AIIMS Nov 2017)

INI-CET 2017 - Pathology INI-CET Practice Questions and MCQs
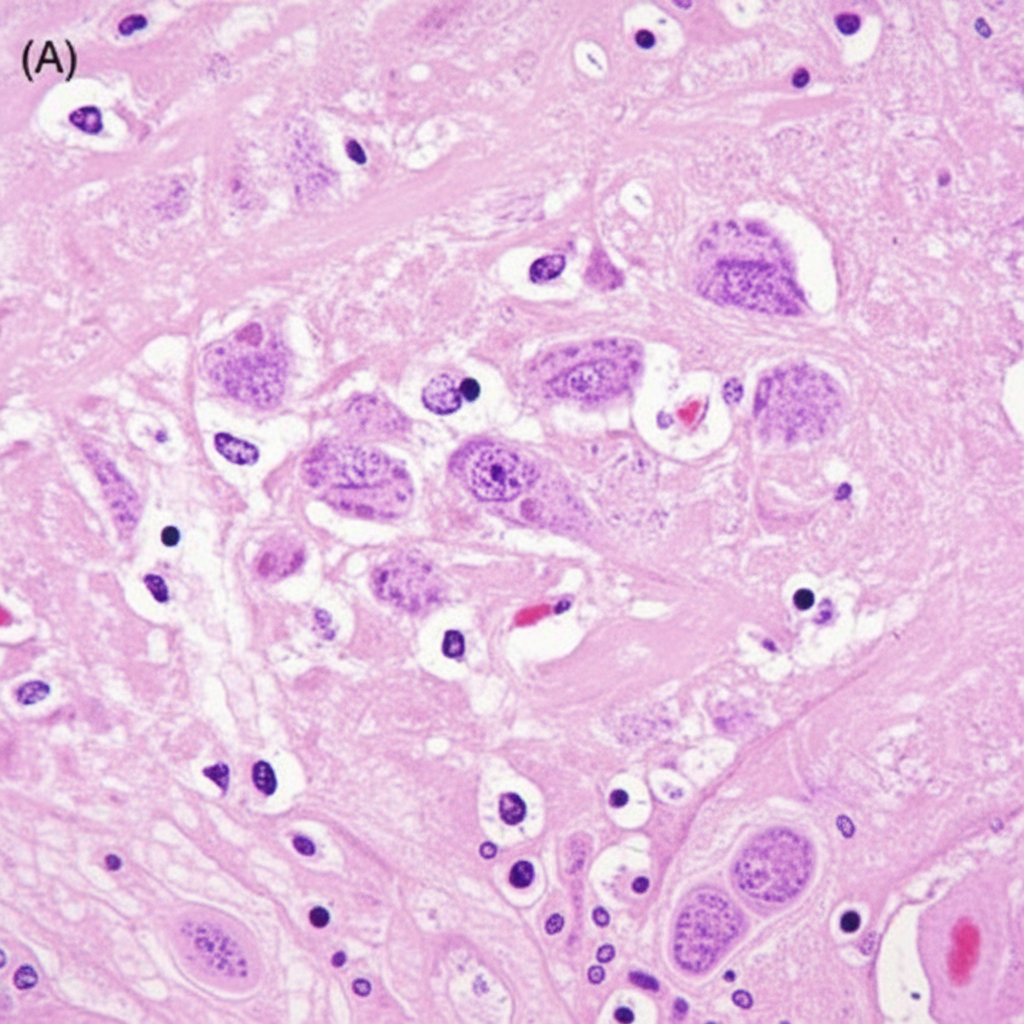
Question 1: The following brain biopsy of patient who presented with marked psychomotor agitation is diagnostic of?
- A. Rabies encephalitis (Correct Answer)
- B. Herpes simplex encephalitis
- C. Creutzfeldt-Jakob disease
- D. Japanese encephalitis
- E. Acute disseminated encephalomyelitis
Explanation: ***Correct: Rabies encephalitis*** - The brain biopsy showing **Negri bodies** (pathognomonic eosinophilic intracytoplasmic inclusions in pyramidal neurons of hippocampus and Purkinje cells of cerebellum) is diagnostic of **rabies encephalitis** - Clinical presentation of **marked psychomotor agitation** is characteristic of the furious form of rabies - Histopathology shows **perivascular lymphocytic cuffing** and neuronal degeneration along with Negri bodies - Rabies is caused by a **neurotropic RNA rhabdovirus** transmitted through animal bites *Incorrect: Herpes simplex encephalitis* - HSV encephalitis primarily affects the **temporal lobes** (hemorrhagic necrotizing encephalitis) - Histology shows **Cowdry type A intranuclear inclusions**, not cytoplasmic Negri bodies - Clinical features include fever, altered sensorium, and temporal lobe signs (olfactory/gustatory hallucinations) *Incorrect: Creutzfeldt-Jakob disease* - CJD is a **prion disease** showing **spongiform changes** (vacuolation) in the brain parenchyma - No viral inclusion bodies are seen - Clinical presentation includes rapidly progressive dementia, myoclonus, and ataxia *Incorrect: Japanese encephalitis* - JE causes **basal ganglia and thalamic involvement** (seen on neuroimaging) - Histology shows **neuronal necrosis and neuronophagia** but no characteristic inclusion bodies like Negri bodies - Clinical features include parkinsonian features and movement disorders *Incorrect: Acute disseminated encephalomyelitis* - ADEM is a **post-infectious demyelinating disease** showing perivenular demyelination - Histology shows demyelination with preservation of axons, not viral inclusions - Usually follows viral infection or vaccination
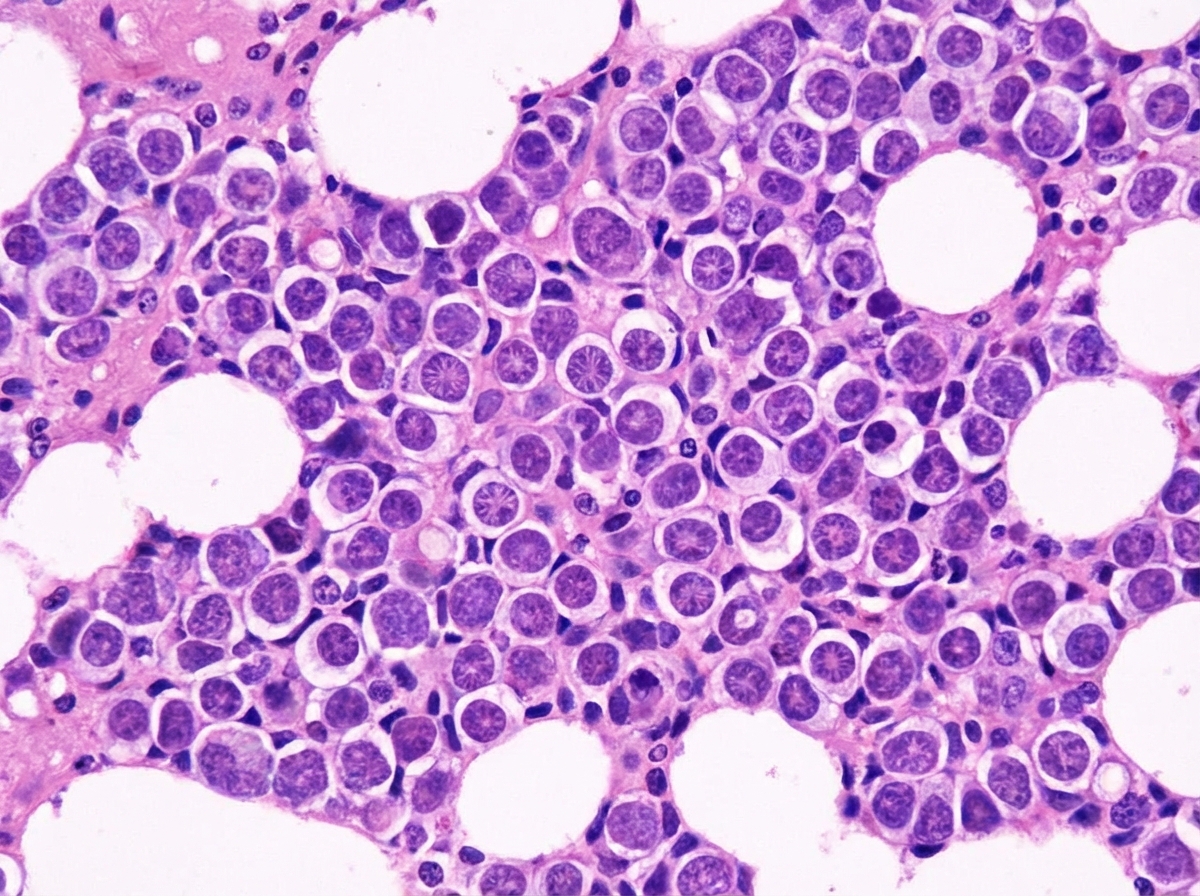
Question 2: A 70-year-old man presents with history of intractable diarrhea. His bone marrow and kidney biopsy are shown below. Which of the following is the most appropriate diagnosis?
- A. Leishmaniasis
- B. Multiple myeloma (Correct Answer)
- C. Lymphoma
- D. Urate nephropathy
- E. Amyloidosis
Explanation: ***Multiple myeloma*** - The combination of intractable diarrhea, bone marrow findings (likely showing **plasma cell proliferation**), and kidney biopsy findings (suggesting **cast nephropathy** or **amyloidosis**) is highly indicative of multiple myeloma [1][3][4]. - **Monoclonal immunoglobulin light chains** produced by plasma cells can cause renal damage and gastrointestinal symptoms like diarrhea [1][2][4]. *Leishmaniasis* - Characterized by **fever**, **splenomegaly**, and **pancytopenia**, with parasites found in macrophages. - While it can affect the bone marrow, it does not typically cause the specific kidney pathology or intractable diarrhea seen in this context. *Lymphoma* - Involves the proliferation of **lymphocytes** and can present with systemic symptoms like fever, weight loss, and lymphadenopathy. - While it can infiltrate the bone marrow and kidneys, it typically does not cause the specific renal casts or amyloid deposition seen in multiple myeloma, nor is intractable diarrhea a primary feature [5]. *Urate nephropathy* - Caused by the deposition of **uric acid crystals** in the renal tubules, leading to acute kidney injury, often in the context of tumor lysis syndrome or gout. - It does not explain the intractable diarrhea or the primary bone marrow pathology of plasma cell proliferation. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 616-617. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 607-608. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 617-618. [4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 618-619. [5] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 606-607.
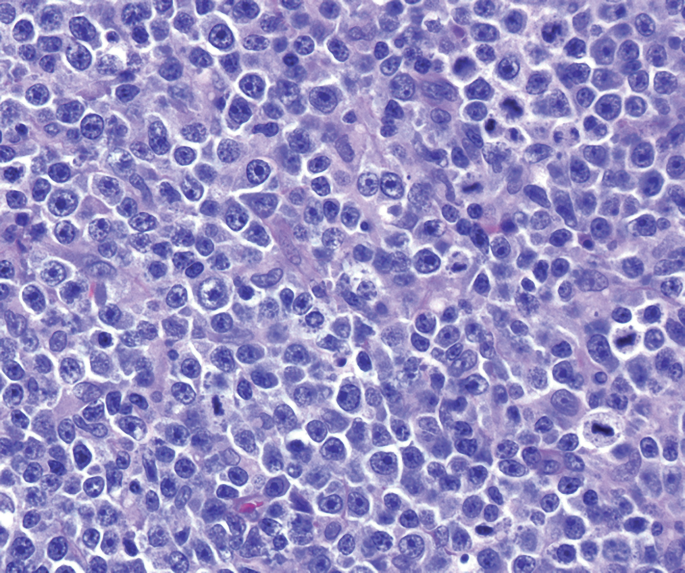
Question 3: A 35-year-old presented with fever. On examination he had enlarged and ulcerated tonsils. Since peripheral smear shows lymphocytosis, monospot test was done which is negative. Tonsillectomy was done and stained section is shown below. Large cells mixed with lymphocytes are seen. The cells are positive for CD20, EBVLMP-1, MUM1, CD 79a and CD 15 negative. The background cells are positive for CD3. Diagnosis is: (AIIMS May 2017)
- A. Infectious mononucleosis
- B. Hodgkin lymphoma
- C. EBV positive- DLBCL
- D. EBV positive- mucocutaneous ulcer (Correct Answer)
- E. Burkitt lymphoma
Explanation: ***EBV positive- mucocutaneous ulcer*** - The presence of **large B-cells (CD20+, CD79a+, MUM1+)** that are **EBV-positive (EBVLMP-1+)** in an ulcerated tonsil, with a **CD15 negative** profile and a background of **CD3+ T-cells**, in a patient with a negative monospot test, is characteristic of **EBV-positive mucocutaneous ulcer**. - This condition is a **polymorphic lymphoproliferative disorder** that typically presents as a localized ulcer and is associated with **immunosuppression** or **immunosenescence**, often resolving with reduced immunosuppression. *Infectious mononucleosis* - While also caused by **EBV** and presenting with **fever** and **enlarged/ulcerated tonsils**, infectious mononucleosis typically has a **positive monospot test** and shows reactive **T-cell lymphocytosis** on peripheral smear [1]. - The large cells in infectious mononucleosis are primarily **atypical T-lymphocytes**, not large B-cells with the described immunophenotype [1]. *Hodgkin lymphoma* - Hodgkin lymphoma is characterized by **Reed-Sternberg cells** and their variants, which are typically **CD15+** and **CD30+**, and **CD20 negative** (or weakly positive), which contradicts the given immunophenotype (CD20+, CD15-) [2][3]. - While some forms of Hodgkin lymphoma are EBV-associated [4], the overall immunophenotype and the description of "large cells mixed with lymphocytes" rather than classic Reed-Sternberg cells make this less likely [2]. *EBV positive- DLBCL* - **EBV-positive diffuse large B-cell lymphoma (DLBCL)** typically presents as a **mass-forming lesion** and is a more aggressive lymphoma. - While it shares the **EBV positivity** and **B-cell immunophenotype (CD20+, CD79a+, MUM1+)**, the clinical presentation as a localized ulcer in a potentially immunocompromised setting, along with the specific mention of "mucocutaneous ulcer," points more towards the distinct entity of EBV-positive mucocutaneous ulcer, which is often a more indolent, self-limiting process. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Infectious Diseases, pp. 369-370. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 614-616. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 556-557. [4] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 616-618.
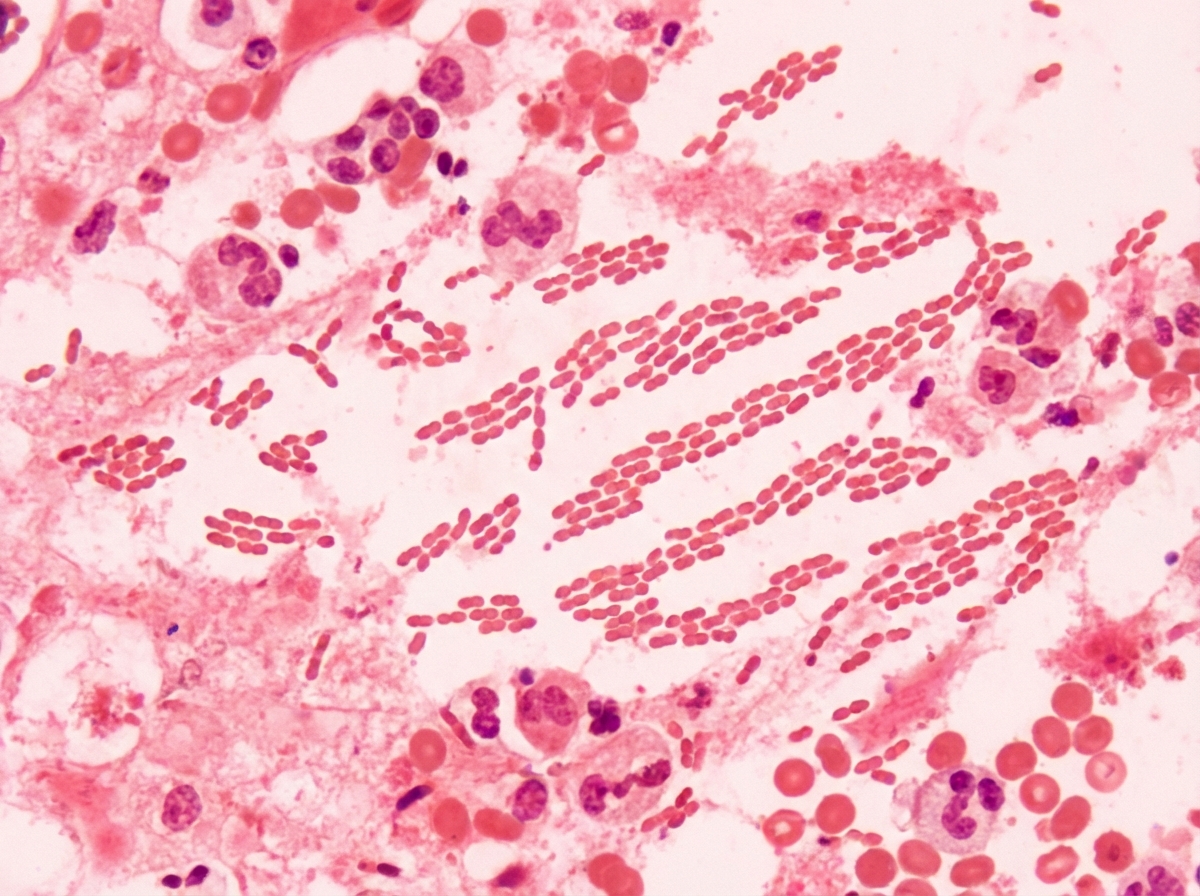
Question 4: The following is a picture from scrapping of genital ulcer. Comment on the diagnosis. (AIIMS May 2017)
- A. Klebsiella granulomatosis
- B. Neisseria gonorrhoea
- C. Chlamydia trachomatis
- D. Treponema pallidum
- E. Haemophilus ducreyi (Correct Answer)
Explanation: ***Hemophilus ducreyi*** - *Hemophilus ducreyi* causes **chancroid**, characterized by painful genital ulcers with ragged, undermined borders and often associated with painful inguinal lymphadenopathy. - Microscopic examination of a smear from the ulcer typically shows **Gram-negative coccobacillary rods** arranged in "school of fish" or "railroad track" patterns. *Klebsiella granulomatosis* - *Klebsiella granulomatosis* (formerly *Calymmatobacterium granulomatis*) causes **donovanosis** (granuloma inguinale), which presents as painless, beefy red, friable ulcers [1]. - Diagnosis is made by identifying **Donovan bodies** (intracellular bipolar-staining rods) in tissue smears or biopsies [1]. *Neisseria gonorrhoea* - *Neisseria gonorrhoea* primarily causes **urethritis** in men and **cervicitis** in women, with purulent discharge. - While it can cause disseminated infection, it typically does not present as a primary genital ulcer. *Chlamydia trachomatis* - *Chlamydia trachomatis* causes **lymphogranuloma venereum (LGV)**, which initially presents as a transient, painless papule or ulcer, often unnoticed. - The characteristic feature of LGV is the subsequent development of **painful inguinal lymphadenopathy** (buboes) and proctitis. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Infectious Diseases, pp. 378-379.
Question 5: The vacutainer shown below is used for collecting sample for? (AIIMS Nov 2017)
- A. Serum electrolytes (Correct Answer)
- B. Serum lactate
- C. Serum cholesterol
- D. Serum uric acid
- E. Coagulation studies
Explanation: ***Serum electrolytes*** - The image shows a **green-top vacutainer**, which typically contains **lithium heparin** as an anticoagulant. - **Lithium heparin** is the preferred anticoagulant for collecting samples for **serum electrolyte** measurements, as it does not interfere with the analysis of ions like sodium, potassium, and chloride. *Serum lactate* - Serum lactate measurements usually require a **gray-top tube** containing **sodium fluoride** and **potassium oxalate** to inhibit glycolysis and stabilize lactate levels. - A green-top tube with lithium heparin is not ideal for lactate analysis due to continued glycolysis in the absence of a glycolysis inhibitor. *Serum cholesterol* - Serum cholesterol, along with other lipid profiles, is typically collected in a **red-top tube** (no additive) or a **SST (serum separator tube)**, which has a gel barrier. - While cholesterol can be measured from a heparinized plasma sample, a plain red-top or SST is more commonly used for routine lipid panels. *Serum uric acid* - Serum uric acid measurement can be performed on a sample collected in a **red-top tube** (no additive) or a **SST (serum separator tube)**. - Although lithium heparin tubes can sometimes be used, plain serum tubes are generally preferred as they yield serum directly without an anticoagulant. *Coagulation studies* - Coagulation studies (PT, PTT, INR) require a **blue-top tube** containing **sodium citrate** as the anticoagulant. - The citrate-to-blood ratio must be precise (1:9) for accurate coagulation testing, making the blue-top tube specifically designed for this purpose. - A green-top tube with heparin cannot be used for coagulation studies as heparin itself is an anticoagulant that would interfere with the test results.