All (115)Anatomy (1)Anatomy (10)Anesthesiology (2)Biochemistry (1)Community Medicine (3)Dermatology (13)ENT (5)Forensic Medicine (3)General Medicine (1)Internal Medicine (7)Internal Medicine (2)Microbiology (10)Obstetrics and Gynecology (3)Ophthalmology (5)Orthopaedics (6)Pathology (9)Pathology (9)Physiology (7)Radiology (5)Surgery (3)Surgery (10)
Q41
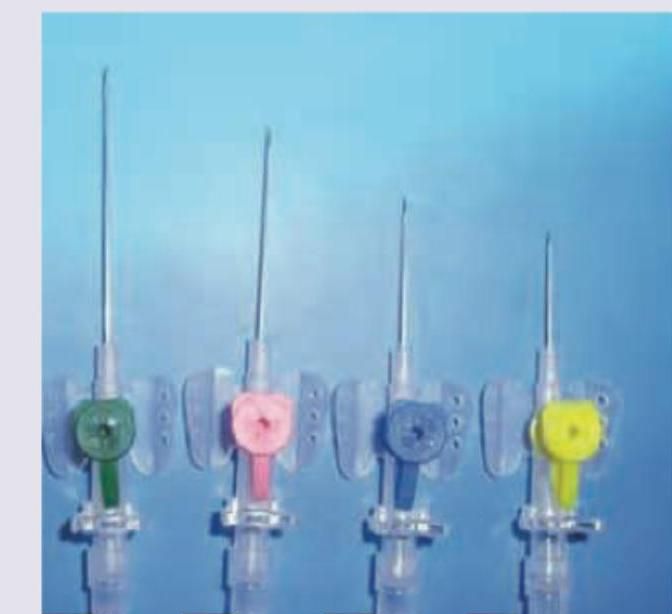
You are asked to put a 22-gauge cannula in a patient. Which of the following cannula will you put?