All (115)Anatomy (1)Anatomy (10)Anesthesiology (2)Biochemistry (1)Community Medicine (3)Dermatology (13)ENT (5)Forensic Medicine (3)General Medicine (1)Internal Medicine (7)Internal Medicine (2)Microbiology (10)Obstetrics and Gynecology (3)Ophthalmology (5)Orthopaedics (6)Pathology (9)Pathology (9)Physiology (7)Radiology (5)Surgery (3)Surgery (10)
Q21
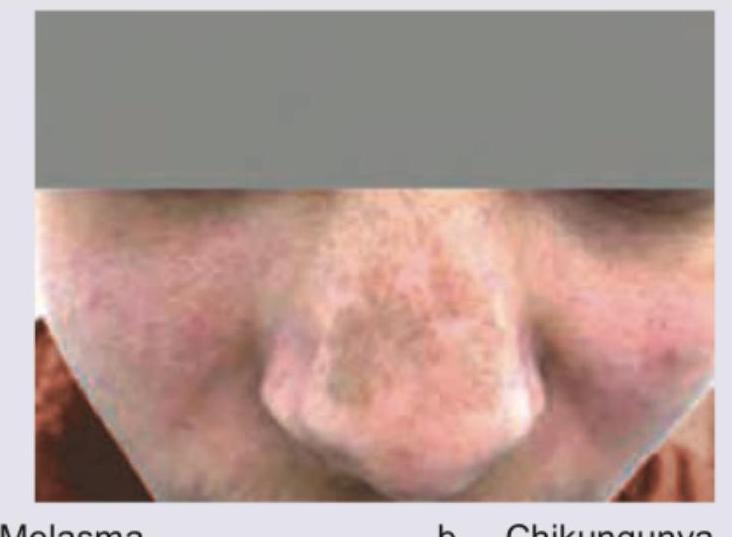
A 30-year-old male presents with joint pain and NSAIDs were prescribed. After one week, joint pain is persisting and he has developed brownish discoloration over nose as shown in the figure. This was due to: (AIIMS Nov 2017)