All (115)Anatomy (1)Anatomy (10)Anesthesiology (2)Biochemistry (1)Community Medicine (3)Dermatology (13)ENT (5)Forensic Medicine (3)General Medicine (1)Internal Medicine (7)Internal Medicine (2)Microbiology (10)Obstetrics and Gynecology (3)Ophthalmology (5)Orthopaedics (6)Pathology (9)Pathology (9)Physiology (7)Radiology (5)Surgery (3)Surgery (10)
Q11
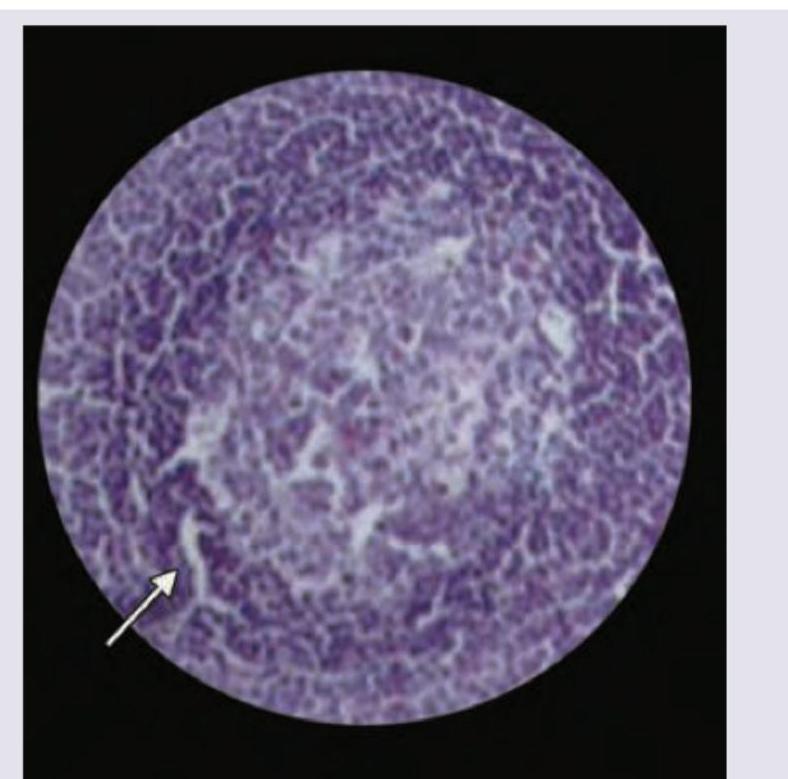
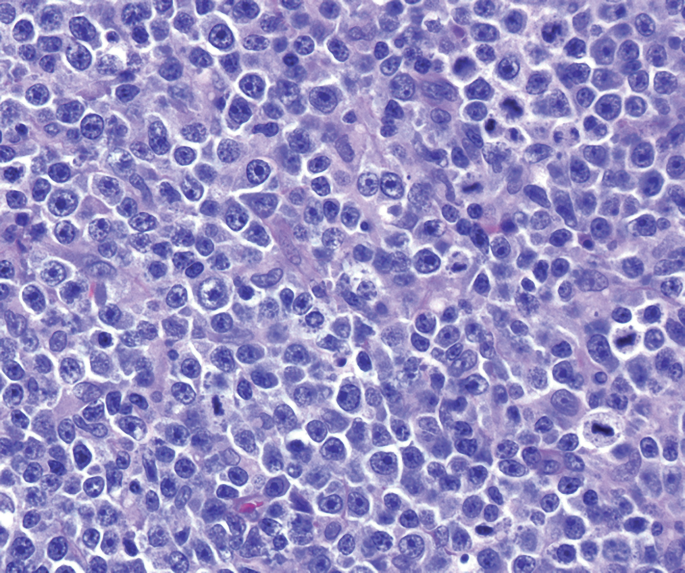
Which of the following area is marked in the histology of lymph node? (AIIMS May 2017)