INI-CET 2017 — Orthopaedics
7 Previous Year Questions with Answers & Explanations
What type of fracture is shown in X-ray of left shoulder?

A 4-year-old boy fell on outstretched hand. X- Ray is shown below. Which blood vessel is most commonly affected?

An elderly patient slipped in the bathroom and sustained injury over the hip joint. X- Ray is shown below. Her attitude of leg will be?

Which position is being tested on the patient in the image shown below?

A patient came with inability to move his 4th and 5th digit and cannot hold pen or paper between his fingers. Which of the following sites shown below is the probable cause of nerve injury to this patient?
Which is the suggested treatment of the lesion shown in the X-ray?

Which of the following is the bone holding instrument used in orthopaedic surgeries?
INI-CET 2017 - Orthopaedics INI-CET Practice Questions and MCQs
Question 1: What type of fracture is shown in X-ray of left shoulder?
- A. Neer classification grade 4
- B. Ideberg classification grade 4 (Correct Answer)
- C. Garden classification grade 3
- D. Schatzker classification grade 5
Explanation: ***Ideberg classification grade 4*** - The X-ray shows a **scapular fracture**, specifically involving the glenoid. Ideberg classification is used for **glenoid fractures**. - An Ideberg grade 4 fracture involves a **transverse fracture below the scapular notch**, separating the load-bearing part of the glenoid from the rest of the scapula, which appears consistent with the image. *Neer classification grade 4* - The **Neer classification** system is used for **proximal humerus fractures**, not scapular fractures. - A grade 4 Neer fracture involves **four part displacement** of the humeral head, greater tuberosity, lesser tuberosity, and humeral shaft. *Garden classification grade 3* - The **Garden classification** system is specifically used for **femoral neck fractures**, which are fractures of the hip. - A Garden grade 3 fracture represents a **complete, displaced fracture of the femoral neck**, distinct from the shoulder injury shown. *Schatzker classification grade 5* - The **Schatzker classification** system is used for **tibial plateau fractures**, which are fractures of the knee joint. - A Schatzker grade 5 fracture involves a **bicondylar fracture** of the tibial plateau, which is severe and impacts the knee, not the shoulder.
Question 2: A 4-year-old boy fell on outstretched hand. X- Ray is shown below. Which blood vessel is most commonly affected?
- A. Ulnar artery
- B. Radial artery (Correct Answer)
- C. Brachial artery
- D. Cubital vein
Explanation: ***Radial artery*** - The X-ray image shows a **supracondylar fracture of the humerus**, which is a common injury in children who fall on an outstretched hand. - While the **brachial artery** runs anterior to the humeral condyles and is the most commonly injured *major* vessel in supracondylar fractures, the **radial artery** is distal to this area and can be affected by subsequent complications like compartment syndrome or direct trauma from displaced fragments, and is a frequently assessed pulse in these injuries to monitor peripheral perfusion. *Ulnar artery* - The ulnar artery is less commonly affected in supracondylar humeral fractures compared to the brachial or radial arteries. - Its anatomical course protects it somewhat from direct trauma in typical fracture displacement patterns. *Brachial artery* - The **brachial artery** is indeed the most commonly injured *major* vessel in supracondylar fractures due to its close proximity to the distal humerus and its anterior course. - However, the question asks for the most commonly affected blood vessel *following* such an injury, and while direct injury to the brachial artery is a concern, assessment of the **radial artery** pulse is critical for evaluating distal perfusion and identifying potential complications like **compartment syndrome**, which affects blood flow through distal arteries like the radial artery. *Cubital vein* - Veins, including the cubital veins, are generally more pliable and less prone to severe injury or occlusion by bone fragments compared to arteries. - While venous compromise can occur, it is less common and less clinically significant in immediate assessment of these fractures compared to arterial injury.
Question 3: An elderly patient slipped in the bathroom and sustained injury over the hip joint. X- Ray is shown below. Her attitude of leg will be?
- A. Shortened, abducted and externally rotated (Correct Answer)
- B. Shortened and abducted
- C. Lengthened and internally rotated
- D. Flexed and adducted and internally rotated
Explanation: ***Shortened, abducted and externally rotated*** - The X-ray image reveals an **intertrochanteric fracture** of the right hip, characterized by a fracture line between the greater and lesser trochanters. - Due to the pull of strong muscles acting on the fractured fragments (e.g., iliopsoas, gluteal muscles), the limb typically assumes a position of **shortening, abduction, and external rotation**. *Shortened and abducted* - While **shortening** and **abduction** are present in intertrochanteric fractures, this answer is incomplete as it misses the crucial component of **external rotation**. - The powerful **external rotators** and the **gravity** acting on the unstable distal fragment contribute significantly to the external rotation. *Lengthened and internally rotated* - This attitude is characteristic of a **posterior hip dislocation**, where the femoral head is driven posteriorly and superiorly, typically leading to limb lengthening and internal rotation. - This is opposite to the typical presentation of an intertrochanteric fracture as seen in the X-ray. *Flexed and adducted and internally rotated* - A flexed, adducted, and internally rotated position is also seen in **posterior hip dislocations**, which is not consistent with the X-ray findings of an intertrochanteric hip fracture. - Hip fractures usually result in some degree of **external rotation** due to the muscle forces.
Question 4: Which position is being tested on the patient in the image shown below?
- A. Internal rotation
- B. External rotation (Correct Answer)
- C. Abduction
- D. Flexion
Explanation: ***External rotation*** - In the image, the patient's hip is flexed and the examiner is rotating the lower leg *medially*, which causes **external rotation** of the hip joint. - This maneuver assesses the range of motion for **external rotation** at the hip. *Internal rotation* - Internal rotation of the hip would involve rotating the lower leg **laterally**, which is the opposite of what is depicted. - This motion brings the front of the thigh closer to the midline when the hip is flexed. *Abduction* - **Abduction** is the movement of the leg away from the midline of the body, which is not being performed in this image. - This movement primarily involves muscles like the **gluteus medius** and **minimus**. *Flexion* - While the hip is maintained in a **flexed position**, the primary motion being tested by the examiner's manipulation is the *rotation* of the femur within the hip socket, not further flexion. - **Flexion** involves lifting the leg towards the torso, often with a bent knee.
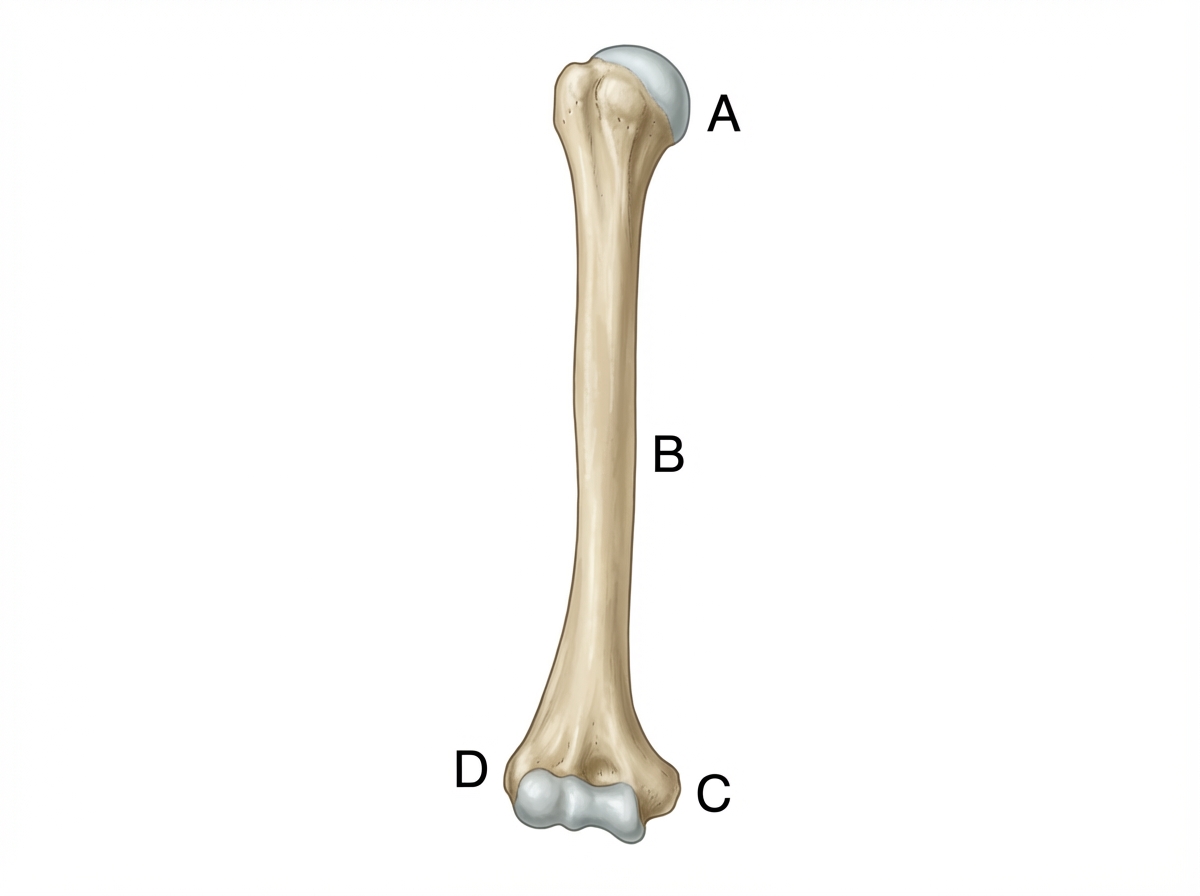
Question 5: A patient came with inability to move his 4th and 5th digit and cannot hold pen or paper between his fingers. Which of the following sites shown below is the probable cause of nerve injury to this patient?
- A. A
- B. B
- C. C (Correct Answer)
- D. D
Explanation: **C** - The symptoms described (inability to move the 4th and 5th digits and difficulty with adduction/abduction of fingers, e.g., holding a pen) are characteristic of **ulnar nerve injury**. - The ulnar nerve passes behind the **medial epicondyle** of the humerus, which corresponds to location **C** in the image, making it vulnerable to injury here. *A* - Location **A** represents the surgical neck of the humerus. Injury here primarily affects the **axillary nerve**, leading to weakness in shoulder abduction and loss of sensation over the deltoid. - This does not explain the specific loss of function in the 4th and 5th digits. *B* - Location **B** represents the mid-shaft of the humerus. Fractures here commonly injure the **radial nerve**, leading to "wrist drop" and sensory loss over the posterior forearm and hand. - This injury pattern does not match the patient's symptoms affecting the ulnar side of the hand. *D* - Location **D** represents the lateral epicondyle of the humerus. This area is associated with conditions like **tennis elbow** (lateral epicondylitis), which involves inflammation of the common extensor origin. - Nerve injuries related to this area typically involve the deep branch of the **radial nerve** (posterior interosseous nerve), leading to weakness in finger and thumb extension, not ulnar nerve symptoms.
Question 6: Which is the suggested treatment of the lesion shown in the X-ray?
- A. Intramedullary nail
- B. Tension band wiring (Correct Answer)
- C. Patellectomy
- D. Above knee cast
Explanation: ***Tension band wiring*** - The X-ray image shows a **transverse patellar fracture** with some displacement, which is well-suited for tension band wiring. - This technique converts tensile forces on the anterior surface of the patella into compressive forces at the fracture site during knee flexion. *Intramedullary nail* - **Intramedullary nailing** is primarily used for **long bone fractures** (e.g., femur, tibia, humerus) and is not appropriate for patellar fractures. - This method is designed to stabilize diaphyseal or metaphyseal fractures in load-bearing long bones by placing a rod within the medullary canal. *Patellectomy* - **Patellectomy** (surgical removal of the patella) is typically reserved for **severely comminuted** or irreparable patellar fractures, or in cases of infection, which is not indicated by the X-ray. - This procedure can lead to significant functional impairment, including reduced quadriceps strength and increased tibiofemoral joint stress. *Above knee cast* - While an **above-knee cast** can provide - An above-knee cast does not provide **sufficient reduction and compression** for displaced patellar fractures, which are subjected to significant tensile forces. - Conservative management is generally reserved for **non-displaced or minimally displaced** patellar fractures where the extensor mechanism remains intact.
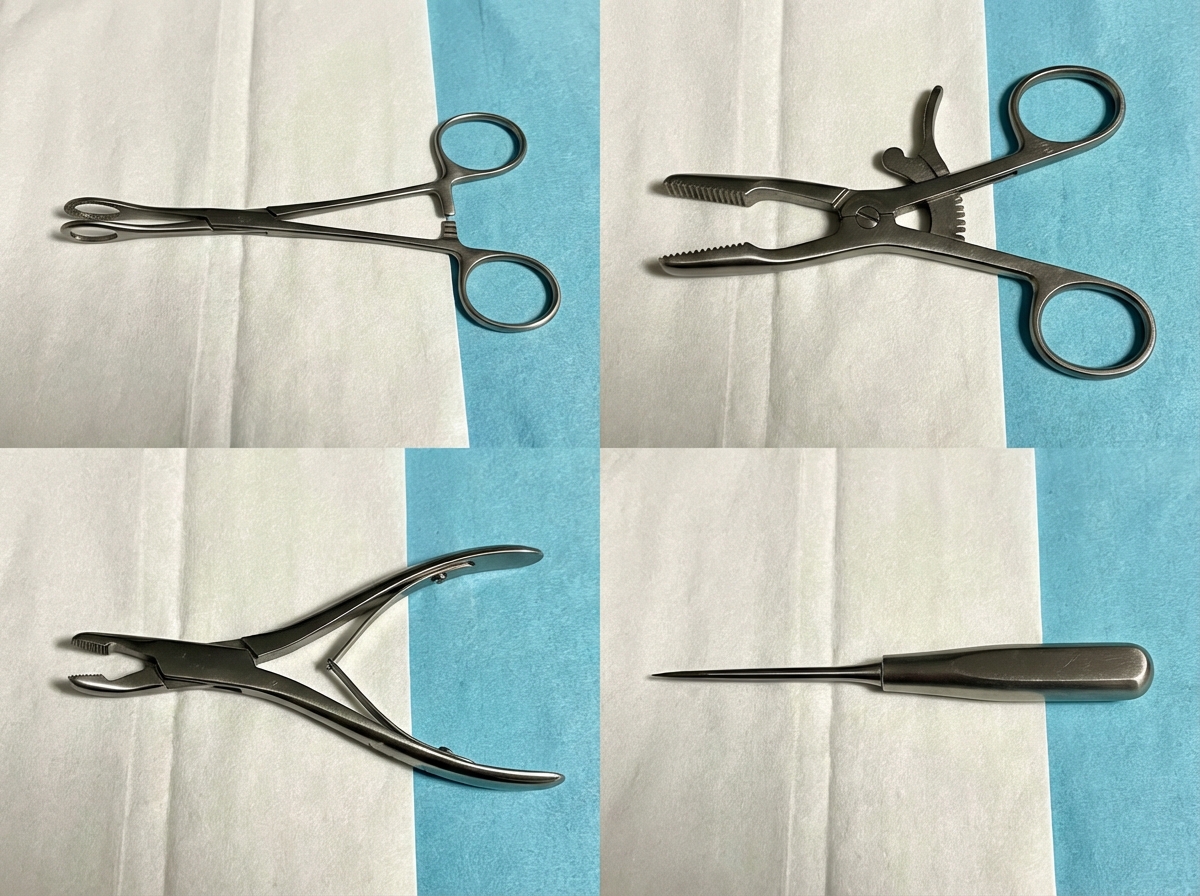
Question 7: Which of the following is the bone holding instrument used in orthopaedic surgeries?
- A. Instrument in upper right quadrant (Correct Answer)
- B. Instrument in upper left quadrant
- C. Instrument in lower left quadrant
- D. Instrument in lower right quadrant
Explanation: ***The image in the upper right quadrant*** - This instrument is a **bone-holding clamp/forceps**, characterized by its robust construction and jaws designed to securely grasp and stabilize bone fragments during orthopedic procedures. - The **ratchet mechanism** visible on the handles allows for maintaining a constant grip on the bone without continuous manual pressure. *The image in the upper left quadrant* - This instrument appears to be a **sponge-holding forceps**, distinguishable by its generally lighter build and oval/circular fenestrated (windowed) tips, which are used to hold sponges or swabs. - Its primary role is for **aseptic preparation** of the surgical site or for absorbing fluids, not for bone manipulation. *The image in the lower left quadrant* - This instrument is a **bone rongeur** or **bone cutter**, designed with sharp, cup-like jaws to bite off small pieces of bone or cartilage. - It is used for **debridement**, shaping bone, or extracting bone fragments, rather than holding them. *The image in the lower right quadrant* - This instrument is a **bone awl** or **trephine**, typically used to create holes or puncture the bone marrow cavity. - It has a pointed, sharp tip and a handle for applying force, but it does not have any mechanism for grasping or holding bone.