All SubjectsAnatomy (1)Anatomy (10)Anesthesiology (2)Biochemistry (1)Community Medicine (3)Dermatology (13)ENT (5)Forensic Medicine (3)General Medicine (1)Internal Medicine (7)Internal Medicine (2)Microbiology (10)Obstetrics and Gynecology (3)Ophthalmology (5)Orthopaedics (6)Pathology (9)Pathology (9)Physiology (7)Radiology (5)Surgery (3)Surgery (10)
Q11
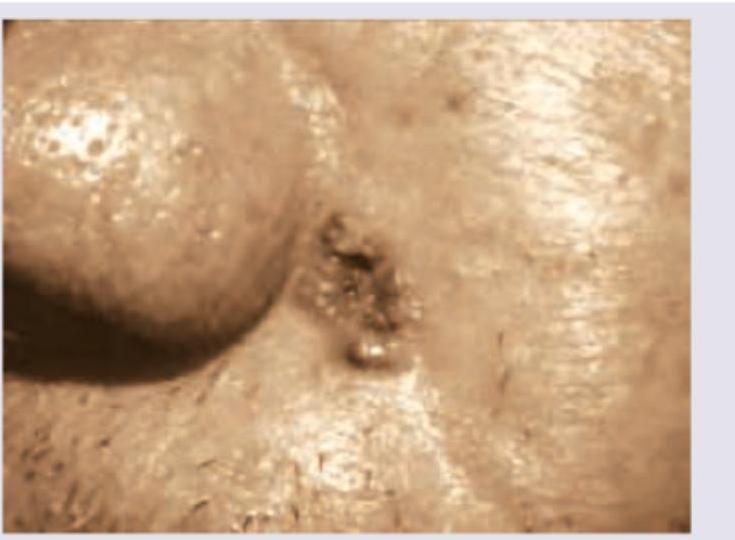
A patient presents with ulcer on the side of the nose, as shown, which bleeds on itching. What is the diagnosis? (AIIMS Nov 2017)
Q12
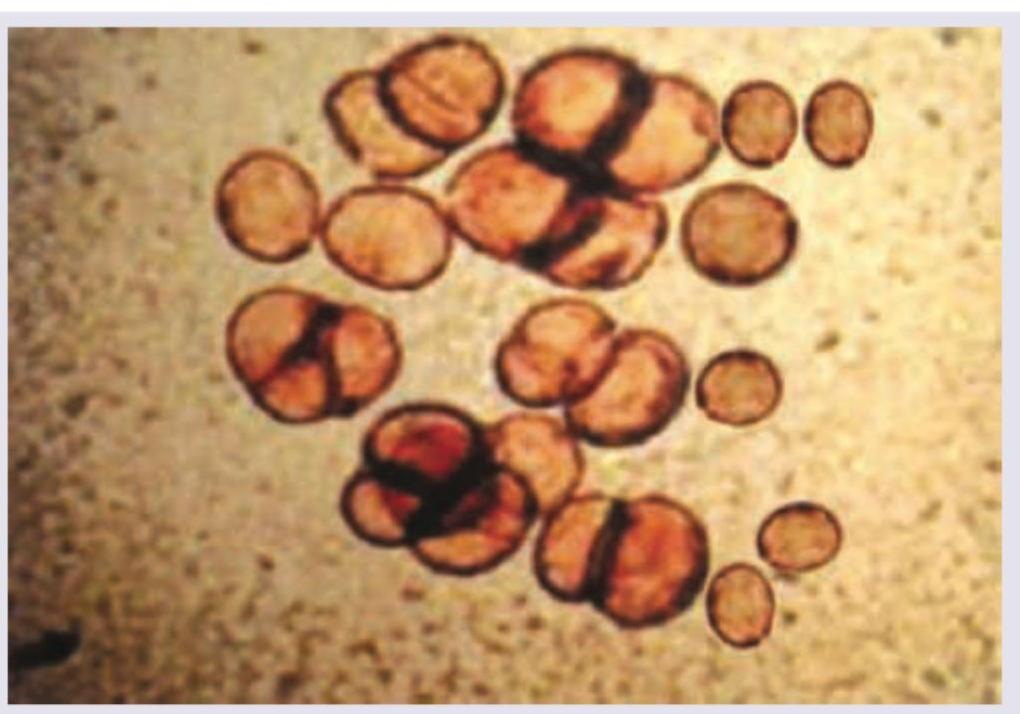
A female had a thorn prick 5 years ago. She presents with development of slowly growing $2 \times 2 \mathrm{~cm}$ verrucous lesion which on KOH mount shows the following image. Diagnosis is: (AIIMS Nov 2017)
Q13
The following presentation is called:
