INI-CET 2017 — Dermatology
12 Previous Year Questions with Answers & Explanations
A 25-year-old lady presents with painful blisters in oral mucosa and skin. Direct immune-fluorescence picture is given below. Which of the following is incorrect about the condition shown?
What is the diagnosis based on the image shown below?
A 30-year-old male presents with joint pain and NSAIDs were prescribed. After one week, joint pain is persisting and he has developed brownish discoloration over nose as shown in the figure. This was due to: (AIIMS Nov 2017)
A child has a pruritic rash as shown below. His mother is an asthmatic. Comment on the diagnosis:

The skin condition shown in the image is associated with?
A middle-aged man came to you with itchy rash caused by the following organism. Identify the condition: (AIIMS Nov 2017)
Identify the condition which is present since birth: (AIIMS May 2017)
A child has been brought with the following scalp lesion with history of itching in scalp and hair loss for past 2 months. Which of the following is useful for diagnosis of this patient? (AIIMS May 2017)

The following patient presented to the OPD with history of hair loss. There was no erythema, scarring or scratching. Diagnosis is:
The image given below shows:

INI-CET 2017 - Dermatology INI-CET Practice Questions and MCQs
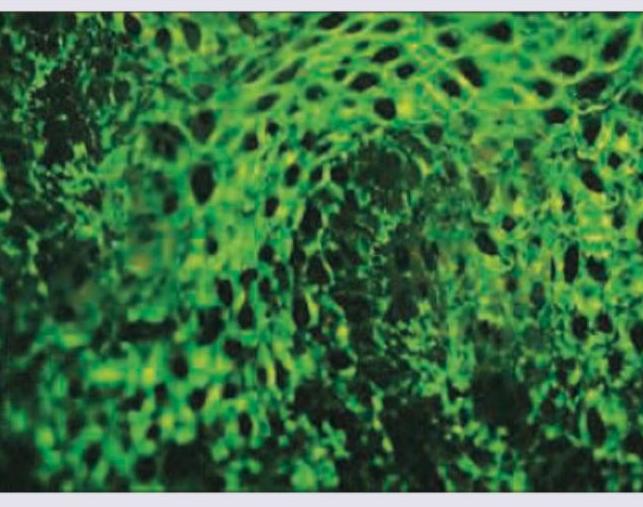
Question 1: A 25-year-old lady presents with painful blisters in oral mucosa and skin. Direct immune-fluorescence picture is given below. Which of the following is incorrect about the condition shown?
- A. Antibodies against hemidesmosomes
- B. Antibodies against desmoglein 1
- C. Antibodies against desmoglein-3
- D. Basement membrane deposition of IgG is the most common DIF picture in bullous lesions (Correct Answer)
Explanation: ***Basement membrane deposition of IgG is the most common DIF picture in bullous lesions*** - This statement is incorrect because the image shows an **intercellular IgG deposition**, characteristic of pemphigus, not basement membrane deposition. - While IgG deposition is common in bullous diseases, its **pattern of deposition** (intercellular vs. basement membrane) is key for diagnosis. *Antibodies against hemidesmosomes* - Antibodies against **hemidesmosomes** are characteristic of **bullous pemphigoid**, which typically presents with tense blisters and subepidermal cleavage. - The direct immunofluorescence (DIF) in bullous pemphigoid would show a **linear deposition of IgG/C3 along the basement membrane zone**, not the intercellular pattern seen in the image. *Antibodies against desmoglein 1* - Antibodies against **desmoglein 1** are seen in **pemphigus foliaceus** and some forms of pemphigus vulgaris affecting mainly the skin. - While associated with pemphigus, the image shows **oral mucosal involvement**, which, when accompanied by skin lesions, often points to a broader autoantibody profile in pemphigus vulgaris (against both Dsg1 and Dsg3). *Antibodies against desmoglein-3* - Antibodies against **desmoglein 3** are characteristic of **pemphigus vulgaris**, especially when **oral mucosal lesions** are prominent. - The presented DIF image shows an **intercellular fishnet pattern of IgG deposition**, which is a hallmark of pemphigus vulgaris, indicating antibodies targeting the desmosomes (which include desmogleins).
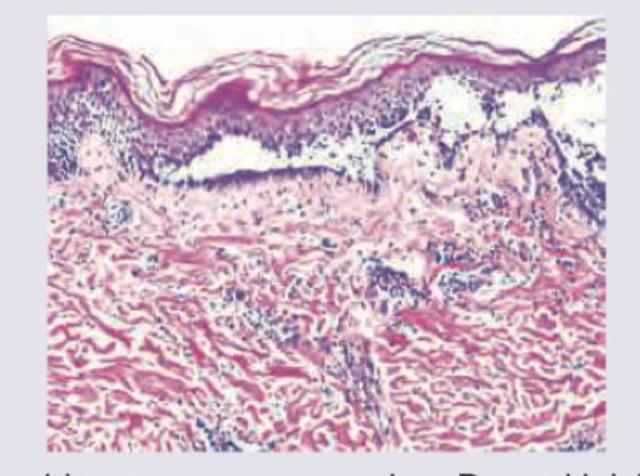
Question 2: What is the diagnosis based on the image shown below?
- A. Pemphigus
- B. Dermal leishmaniasis
- C. Mycosis fungoides (Correct Answer)
- D. Psoriasis
Explanation: ***Mycosis fungoides*** - The image exhibits **Pautrier microabscesses**, which are collections of atypical lymphocytes within the epidermis, a hallmark of mycosis fungoides. - There is also a **band-like infiltrate of atypical lymphocytes** in the upper dermis, characteristic of this cutaneous T-cell lymphoma. *Pemphigus* - Pemphigus is characterized by **intraepidermal blistering due to acantholysis** (loss of cohesion between keratinocytes), which is not seen in this image. - Histology would show separated keratinocytes, often with a "tombstone" appearance of basal cells, and **no Pautrier microabscesses**. *Dermal leishmaniasis* - Dermal leishmaniasis is caused by _Leishmania_ parasites and typically presents with a **dermal infiltrate rich in macrophages** containing intracellular amastigotes. - The image does not show these features; instead, it shows an atypical lymphoid infiltrate. *Psoriasis* - Psoriasis typically shows **acanthosis (epidermal hyperplasia)** with elongation of rete ridges, **parakeratosis**, and **Munro microabscesses** (neutrophilic collections in the stratum corneum). - While there is some epidermal thickening, the distinct Pautrier microabscesses and atypical lymphoid infiltrate are not features of psoriasis.
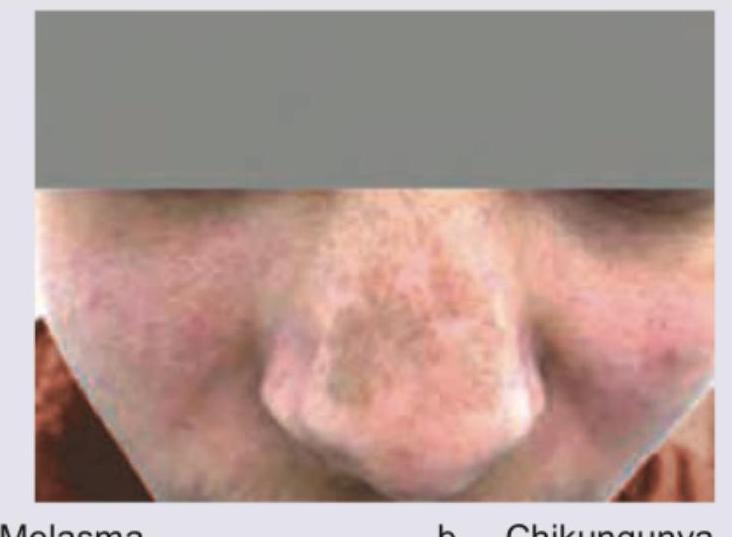
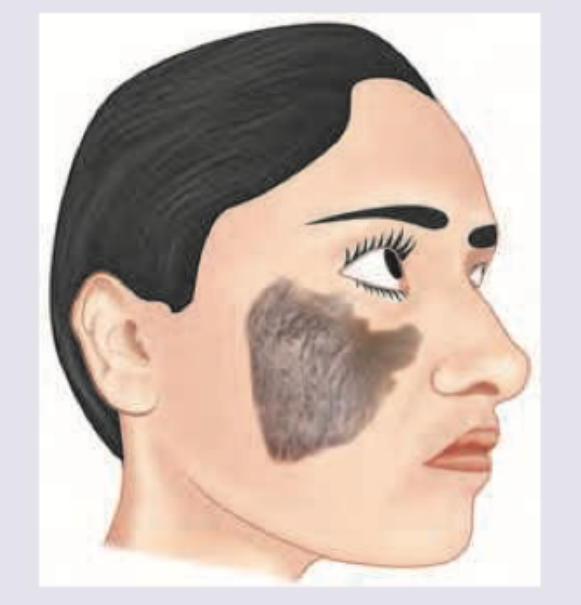
Question 3: A 30-year-old male presents with joint pain and NSAIDs were prescribed. After one week, joint pain is persisting and he has developed brownish discoloration over nose as shown in the figure. This was due to: (AIIMS Nov 2017)
- A. Melasma
- B. Chikungunya
- C. Fixed drug eruption (Correct Answer)
- D. Dengue
Explanation: ***Fixed drug eruption*** - A **fixed drug eruption (FDE)** is a localized cutaneous drug reaction that characteristically **recurs at the same site** upon re-exposure to the offending drug, presenting as well-demarcated erythematous patches, plaques, vesicles, or bullae that heal with **post-inflammatory hyperpigmentation** (brownish discoloration). - NSAIDs (particularly phenylbutazone, oxicams, and diclofenac) are among the **most common causes** of fixed drug eruption. The scenario describes **brownish discoloration on the nose** appearing one week after NSAID use, which represents the characteristic hyperpigmentation phase of FDE. - The **timing** (within 1-2 weeks of drug exposure), **localized distribution** (single site on nose), and **clinical presentation** (brownish patch after medication) are pathognomonic for fixed drug eruption. *Melasma* - **Melasma** causes symmetrical, patchy hyperpigmentation typically on sun-exposed facial areas (malar eminences, forehead, upper lip) and is associated with **hormonal factors** (pregnancy, oral contraceptives) or chronic sun exposure. - It develops **gradually over months**, not acutely within one week of medication use, and shows a bilateral, symmetrical pattern rather than a localized unilateral presentation. *Chikungunya* - **Chikungunya** is a mosquito-borne viral infection presenting with acute fever, severe polyarthralgia, and a **maculopapular or petechial rash** that appears during the febrile phase. - The rash is typically generalized and erythematous, not a localized brownish hyperpigmented patch. While joint pain is prominent, the temporal relationship with NSAID use and the specific skin finding (brownish discoloration post-medication) point away from viral arthritis. *Dengue* - **Dengue** fever presents with high fever, retro-orbital headache, myalgia, and a characteristic **blanching maculopapular or petechial rash** appearing 2-5 days after fever onset. - The rash is typically generalized and associated with systemic features (fever, thrombocytopenia, bleeding manifestations), not a localized brownish patch appearing after NSAID therapy without fever.
Question 4: A child has a pruritic rash as shown below. His mother is an asthmatic. Comment on the diagnosis:
- A. Seborrheic dermatitis
- B. Atopic dermatitis (Correct Answer)
- C. Allergic contact dermatitis
- D. Erysipelas
Explanation: ***Atopic dermatitis*** - The image shows a classic presentation of **eczematous rash** in the **flexural areas** (knees), which is characteristic of atopic dermatitis. - The history of a **mother with asthma** suggests an **atopic diathesis**, increasing the likelihood of atopic dermatitis in the child due to its strong genetic component and association with other atopic conditions (asthma, allergic rhinitis). *Seborrheic dermatitis* - Typically presents as **greasy, yellowish scales** on an erythematous base, commonly affecting the scalp, face (eyebrows, nasolabial folds), and chest. - While it can occur in infants ("cradle cap"), its morphology and locations are distinct from the rash seen in the image. *Allergic contact dermatitis* - This rash would typically be localized to areas of direct contact with an **allergen** and would not necessarily show the typical flexural distribution seen in the image. - It often presents with more acute **vesicles, bullae, and intense pruritus** strictly limited to the exposure site. *Erysipelas* - Erysipelas is a **superficial bacterial skin infection** characterized by a **well-demarcated, erythematous, raised, and warm plaque**, often with systemic symptoms like fever and chills. - The rash in the image does not present with the characteristic features of an acute bacterial infection.
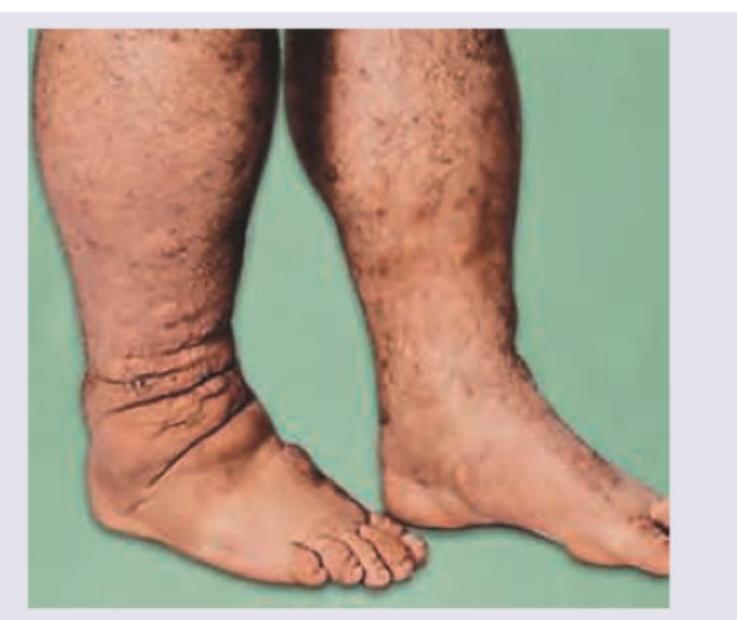
Question 5: The skin condition shown in the image is associated with?
- A. Diabetes mellitus (Correct Answer)
- B. Hypothyroidism
- C. Hyperthyroidism
- D. Sarcoidosis
Explanation: ***Diabetes mellitus*** - The image shows **diabetic dermopathy** (also known as "shin spots"), which presents as hyperpigmented, atrophic macules or papules, usually on the shins. This condition is a common cutaneous manifestation of **diabetes mellitus**. - Other dermatological conditions associated with diabetes include **necrobiosis lipoidica diabeticorum**, **acanthosis nigricans**, and **erythrasma**, which are important to recognize in patients with diabetes. *Hypothyroidism* - Hypothyroidism is associated with **myxedema**, which typically manifests as non-pitting edema, dry and coarse skin, and hair loss. - While it can cause skin changes, it does not typically present with the pigmented, atrophic lesions seen in the image. *Hyperthyroidism* - Hyperthyroidism can cause skin changes such as **pretibial myxedema** (a specific form of localized skin thickening, typically on the shins, that is often associated with Graves' disease) and warm, moist skin due to increased metabolism. - The lesions shown in the image are not consistent with the typical presentation of pretibial myxedema or other hyperthyroid skin manifestations. *Sarcoidosis* - Sarcoidosis can present with various skin lesions, including **erythema nodosum**, lupus pernio, plaques, and papules. - The skin changes seen in the image, characterized by small, atrophic, hyperpigmented macules, do not fit the typical pattern of cutaneous sarcoidosis.
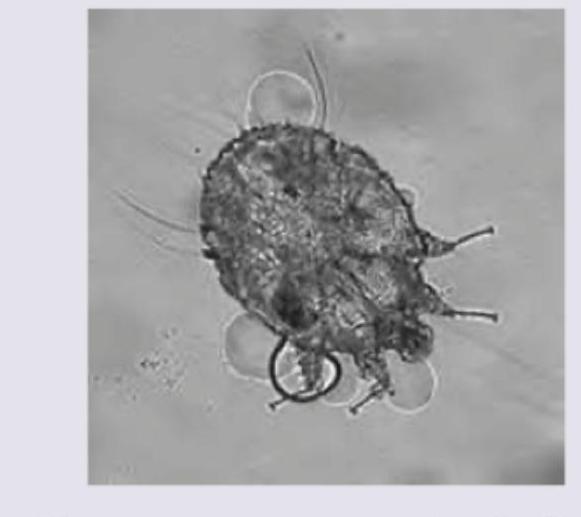
Question 6: A middle-aged man came to you with itchy rash caused by the following organism. Identify the condition: (AIIMS Nov 2017)
- A. Insect bite reaction
- B. Scabies (Correct Answer)
- C. Pediculosis
- D. Tinea cruris
Explanation: ***Scabies*** - The image provided shows **Sarcoptes scabiei**, the scabies mite, which is the causative organism for scabies. - Scabies is characterized by an **intensely itchy rash**, often worse at night, and typical burrows in the skin. *Pediculosis* - Pediculosis is caused by lice (e.g., **Pediculus humanus** or **Pthirus pubis**), which are distinct in appearance from the mite shown. - While also causing an itchy rash, the morphology of the causative agent in the image does not match that of a louse. *Insect bite reaction* - An insect bite reaction is a broad term for inflammatory responses to bites from various insects, but the image specifically identifies the **causative organism**. - The organism shown is a mite, which can cause an insect bite reaction, but scabies is the specific condition caused by this particular mite. *Tinea cruris* - Tinea cruris is a **fungal infection** of the groin, commonly known as jock itch. - The image displays a **mite**, not a fungus, making Tinea cruris an incorrect diagnosis.
Question 7: Identify the condition which is present since birth: (AIIMS May 2017)
- A. Epidermal verrucous nevus
- B. Melano-acanthoma
- C. Malignant melanoma
- D. Congenital nevus (Correct Answer)
Explanation: **Correct: *Congenital nevus*** - A congenital nevus is a **melanocytic nevus** that is present at **birth** or appears shortly thereafter, characterized by a proliferation of **melanocytes** in the skin - These nevi can vary in size and appearance, often appearing as darkly pigmented, sometimes hairy patches - By definition, this is the condition present since birth as asked in the question *Incorrect: Epidermal verrucous nevus* - An **epidermal verrucous nevus** is a common **hamartoma of the epidermis** that can be present at birth or develop in early childhood, characterized by **verrucous** (wart-like) or ridge-like papules and plaques - While it can be congenital, its distinctive **verrucous texture** (wart-like appearance) differentiates it from the smooth, pigmented melanocytic lesion - Not the best answer as the question specifically asks for a condition present since birth, and congenital nevus is more definitively congenital *Incorrect: Melano-acanthoma* - **Melano-acanthoma** is a rare, benign, typically **pigmented lesion** that usually arises in older adults, often on the **trunk or face** - Its late-onset presentation (typically in adulthood) makes it unlikely to be present since birth - This is an acquired condition, not congenital *Incorrect: Malignant melanoma* - **Malignant melanoma** is a serious form of **skin cancer** that typically develops from pre-existing moles or new lesions, most commonly in adulthood - While congenital nevi can rarely undergo malignant transformation into melanoma, melanoma itself is generally not present at birth - Characterized by rapid changes in size, shape, or color (ABCDE criteria), which distinguishes it from stable congenital lesions
Question 8: A child has been brought with the following scalp lesion with history of itching in scalp and hair loss for past 2 months. Which of the following is useful for diagnosis of this patient? (AIIMS May 2017)
- A. Gram stain
- B. KOH mount (Correct Answer)
- C. Slit skin smear
- D. Tzanck smear
Explanation: ***KOH mount*** - The image shows a **patch of hair loss** with visible scaling on the scalp, along with a history of itching, which is highly suggestive of **tinea capitis (ringworm of the scalp)**. - A **KOH (potassium hydroxide) mount** is the most common and effective initial diagnostic test for fungal infections of the skin, hair, and nails, as it helps visualize fungal elements (hyphae and spores). *Gram stain* - **Gram stain** is primarily used to identify **bacterial infections** by differentiating bacteria based on their cell wall composition. - It is not useful for diagnosing **fungal infections** like tinea capitis. *Slit skin smear* - A **slit skin smear** is a diagnostic technique mainly used for the detection of **Mycobacterium leprae** in cases of **leprosy**. - It is not relevant for diagnosing common fungal scalp infections. *Tzanck smear* - A **Tzanck smear** is used to identify **multinucleated giant cells** and **acantholytic cells**, characteristic findings in **herpes simplex**, **varicella zoster**, and other blistering viral conditions. - This method is not used for the diagnosis of **fungal infections** of the scalp.
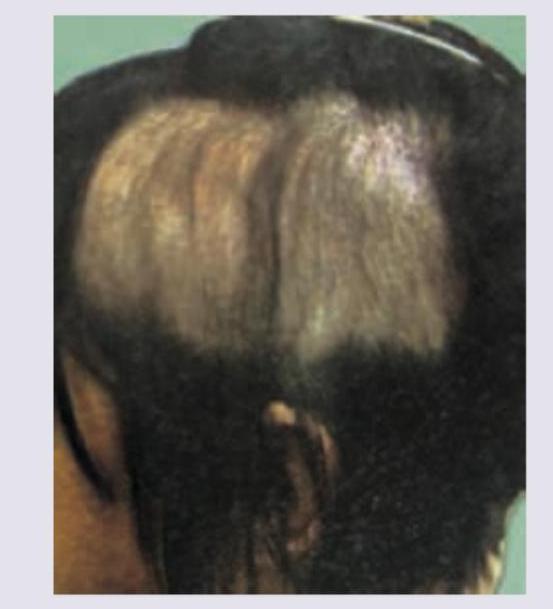
Question 9: The following patient presented to the OPD with history of hair loss. There was no erythema, scarring or scratching. Diagnosis is:
- A. Trichotillomania
- B. Alopecia areata (Correct Answer)
- C. Telogen effluvium
- D. Tinea infection
Explanation: ***Alopecia areata*** - The image shows **well-demarcated patches of hair loss** with no signs of inflammation or scarring, which is characteristic of alopecia areata. - This condition is an **autoimmune disorder** where the immune system attacks hair follicles, leading to patchy hair loss. - Classic presentation includes **smooth, round patches** with no erythema or scarring. *Trichotillomania* - This condition involves **compulsive hair pulling**, which typically results in **irregularly shaped patches of hair loss** with hairs of varying lengths. - Hair loss in trichotillomania often shows **broken hair shafts** and may be associated with signs of trauma or follicular damage. - The absence of scratching/pulling behavior and the well-defined patches make this less likely. *Telogen effluvium* - Telogen effluvium presents as **diffuse hair shedding** (increased shedding of resting phase hairs) rather than the distinct, localized patches seen in the image. - It usually follows a **stressful event** (e.g., illness, surgery, childbirth) and there's no visible inflammation or scarring. - Would not present as well-demarcated patches. *Tinea infection* - Tinea capitis (ringworm of the scalp) would typically present with **erythema, scaling, inflammation**, and sometimes pustules or kerion formation within the patches of hair loss. - The patches of hair loss in tinea infections often show **broken hairs** or "black dots" where hairs have broken off at the scalp surface. - The **absence of erythema** in this case rules out tinea infection.
Question 10: The image given below shows:
- A. Cutaneous horn (Correct Answer)
- B. Papilloma
- C. Cock's peculiar tumor
- D. Glomus tumor
Explanation: ***Cutaneous horn (Cornu cutaneum)*** - The image distinctly shows an **exophytic, conical, or cylindrical lesion** composed of compact keratin, resembling an animal's horn, which is characteristic of a cutaneous horn. - A cutaneous horn is a **clinical descriptive term** for a keratinous projection and is NOT of sebaceous origin; it can arise from various underlying conditions including **seborrheic keratosis, viral warts, actinic keratosis**, or benign lesions. - Importantly, cutaneous horns can rarely **harbor squamous cell carcinoma** or other underlying skin cancers at their base (up to 20% have underlying malignancy), necessitating biopsy and histopathological examination. *Papilloma* - A papilloma is a general term for a **benign epithelial tumor** growing exophytically in a frond-like or papillary pattern, often softer and not typically forming such a dense, hardened projection. - While some papillomas can be keratotic, they usually lack the extreme **horn-like appearance** made of densely packed keratin seen in the image. *Cock's peculiar tumor* - Cock's peculiar tumor, also known as a **calcifying epithelioma of Malherbe** or **pilomatricoma**, is typically a firm, deep-seated nodule arising from hair matrix cells, often with a bluish or reddish hue. - It does not present as a **hard, projecting, horn-like accumulation of keratin** on the skin surface. *Glomus tumor* - A glomus tumor is a rare, **benign neurovascular tumor** typically found in the digits (especially subungual), characterized by exquisite pain, cold sensitivity, and often present as a small, reddish-blue nodule. - Its presentation is distinctly different from the **hyperkeratotic cutaneous projection** shown and does not form a horn-like structure.