INI-CET 2017
104 Previous Year Questions with Answers & Explanations
Dermatology
2 questionsA 25-year-old lady presents with painful blisters in oral mucosa and skin. Direct immune-fluorescence picture is given below. Which of the following is incorrect about the condition shown?
What is the diagnosis based on the image shown below?
INI-CET 2017 - Dermatology INI-CET Practice Questions and MCQs
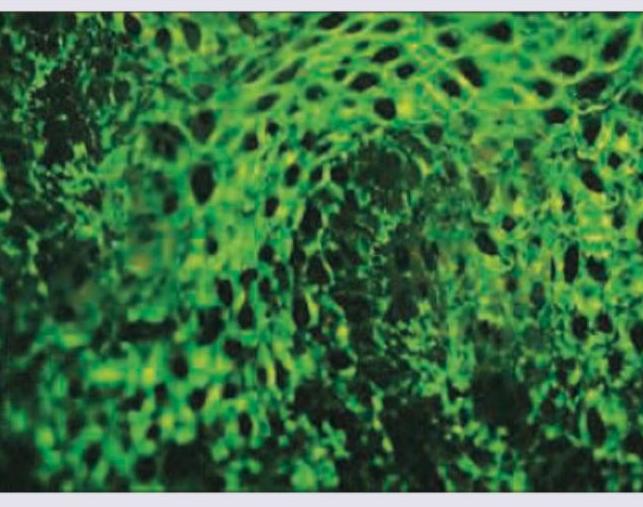
Question 1: A 25-year-old lady presents with painful blisters in oral mucosa and skin. Direct immune-fluorescence picture is given below. Which of the following is incorrect about the condition shown?
- A. Antibodies against hemidesmosomes
- B. Antibodies against desmoglein 1
- C. Antibodies against desmoglein-3
- D. Basement membrane deposition of IgG is the most common DIF picture in bullous lesions (Correct Answer)
Explanation: ***Basement membrane deposition of IgG is the most common DIF picture in bullous lesions*** - This statement is incorrect because the image shows an **intercellular IgG deposition**, characteristic of pemphigus, not basement membrane deposition. - While IgG deposition is common in bullous diseases, its **pattern of deposition** (intercellular vs. basement membrane) is key for diagnosis. *Antibodies against hemidesmosomes* - Antibodies against **hemidesmosomes** are characteristic of **bullous pemphigoid**, which typically presents with tense blisters and subepidermal cleavage. - The direct immunofluorescence (DIF) in bullous pemphigoid would show a **linear deposition of IgG/C3 along the basement membrane zone**, not the intercellular pattern seen in the image. *Antibodies against desmoglein 1* - Antibodies against **desmoglein 1** are seen in **pemphigus foliaceus** and some forms of pemphigus vulgaris affecting mainly the skin. - While associated with pemphigus, the image shows **oral mucosal involvement**, which, when accompanied by skin lesions, often points to a broader autoantibody profile in pemphigus vulgaris (against both Dsg1 and Dsg3). *Antibodies against desmoglein-3* - Antibodies against **desmoglein 3** are characteristic of **pemphigus vulgaris**, especially when **oral mucosal lesions** are prominent. - The presented DIF image shows an **intercellular fishnet pattern of IgG deposition**, which is a hallmark of pemphigus vulgaris, indicating antibodies targeting the desmosomes (which include desmogleins).
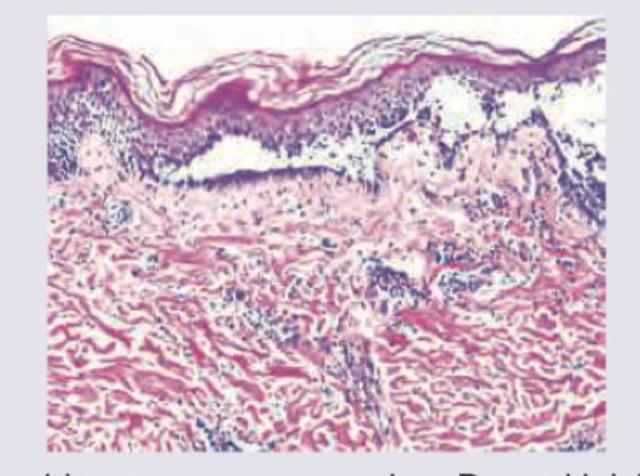
Question 2: What is the diagnosis based on the image shown below?
- A. Pemphigus
- B. Dermal leishmaniasis
- C. Mycosis fungoides (Correct Answer)
- D. Psoriasis
Explanation: ***Mycosis fungoides*** - The image exhibits **Pautrier microabscesses**, which are collections of atypical lymphocytes within the epidermis, a hallmark of mycosis fungoides. - There is also a **band-like infiltrate of atypical lymphocytes** in the upper dermis, characteristic of this cutaneous T-cell lymphoma. *Pemphigus* - Pemphigus is characterized by **intraepidermal blistering due to acantholysis** (loss of cohesion between keratinocytes), which is not seen in this image. - Histology would show separated keratinocytes, often with a "tombstone" appearance of basal cells, and **no Pautrier microabscesses**. *Dermal leishmaniasis* - Dermal leishmaniasis is caused by _Leishmania_ parasites and typically presents with a **dermal infiltrate rich in macrophages** containing intracellular amastigotes. - The image does not show these features; instead, it shows an atypical lymphoid infiltrate. *Psoriasis* - Psoriasis typically shows **acanthosis (epidermal hyperplasia)** with elongation of rete ridges, **parakeratosis**, and **Munro microabscesses** (neutrophilic collections in the stratum corneum). - While there is some epidermal thickening, the distinct Pautrier microabscesses and atypical lymphoid infiltrate are not features of psoriasis.
Forensic Medicine
1 questionsA person is not criminally responsible for their actions if, at the time of committing the act, they are unable to know the nature of the act or understand that it is either wrong or contrary to the law due to unsoundness of mind.
INI-CET 2017 - Forensic Medicine INI-CET Practice Questions and MCQs
Question 1: A person is not criminally responsible for their actions if, at the time of committing the act, they are unable to know the nature of the act or understand that it is either wrong or contrary to the law due to unsoundness of mind.
- A. McNaughten rule (Correct Answer)
- B. Irresistible impulse test
- C. Currens rule
- D. Durham's rule
Explanation: ***McNaughten rule*** - This rule states that a person is not criminally responsible if, at the time of committing the act, they were suffering from a **disease of the mind** that rendered them unable to know the **nature and quality of the act** or that it was wrong. - It focuses on the defendant's **cognitive capacity** to understand their actions and their moral or legal implications. *Durham's rule* - This rule, from the 1954 case *Durham v. United States*, states that an accused is not criminally responsible if their unlawful act was the **product of mental disease or defect**. - It is broader than McNaughten, focusing on the causal link between mental illness and the crime, but was criticized for its vagueness and has been largely replaced. *Currens rule* - From the 1961 case *United States v. Currens*, this test states that a defendant is not criminally responsible if they lacked **substantial capacity** to conform their conduct to the requirements of law due to mental disease or defect. - It is similar to the ALI (American Law Institute) test and focuses on both cognitive and volitional impairment, but is not widely used in Indian forensic practice. *Irresistible impulse test* - This test is a supplement to the McNaughten rule, asserting that a defendant is not criminally responsible if a mental disease prevented them from resisting an impulse to commit the crime, even if they knew the act was wrong. - It focuses on the defendant's **volitional capacity** – their ability to control their conduct.
Internal Medicine
1 questionsA middle-aged woman with a history of backache who underwent a Schober test and tested positive, and who also has hyperpigmented nose and ears, is most likely diagnosed with:
INI-CET 2017 - Internal Medicine INI-CET Practice Questions and MCQs
Question 1: A middle-aged woman with a history of backache who underwent a Schober test and tested positive, and who also has hyperpigmented nose and ears, is most likely diagnosed with:
- A. Ankylosing spondylitis
- B. Degenerative disc disease
- C. Ochronosis (Correct Answer)
- D. Fluorosis
Explanation: ***Ochronosis*** - **Hyperpigmentation of the nose and ears** (due to homogentisic acid accumulation) along with **backache** and a positive **Schober test** (indicating spinal inflexibility from ochronotic arthropathy) are classic features of ochronosis. - This inherited disorder results from a deficiency of **homogentisic acid oxidase**, leading to the accumulation of homogentisic acid. *Ankylosing spondylitis* - While **backache** and a positive **Schober test** (indicating axial skeleton involvement) are characteristic of ankylosing spondylitis, it does not typically present with **hyperpigmented nose and ears**. - **HLA-B27 positivity** and inflammatory back pain improving with activity are key differentiating features not mentioned. *Degenerative disc disease* - This condition is characterized by **chronic backache** due to age-related changes in the intervertebral discs but does not cause **hyperpigmentation of the nose and ears**. - A **positive Schober test** is less specific for degenerative disc disease and is more indicative of widespread spinal stiffness. *Fluorosis* - While severe fluorosis can lead to **skeletal changes** and pain mimicking arthritis, it is primarily associated with **dental mottling** and does not cause characteristic hyperpigmentation of the nose and ears. - มัน usually results from excessive fluoride intake, often from contaminated drinking water.
Pathology
6 questionsA patient with a depressive illness is brought to casualty with acute breathlessness. X-ray shows diffuse infiltrates in right middle lobe and right lower lobe. The patient expired. The lung specimen on biopsy shows:
An 18-year-old male with severe effort intolerance and dyspnea is found to have left atrial enlargement on Chest X-ray. Histopathological examination shows:
The following brain biopsy of patient who presented with marked psychomotor agitation is diagnostic of?
A 70-year-old man presents with history of intractable diarrhea. His bone marrow and kidney biopsy are shown below. Which of the following is the most appropriate diagnosis?
Identify the stain shown in the liver section.
A 50-year-old male presents with colicky abdominal pain and recurrent bloody diarrhea. Colonoscopy shows geographical ulcers. Histopathology is shown below. Diagnosis is:
INI-CET 2017 - Pathology INI-CET Practice Questions and MCQs
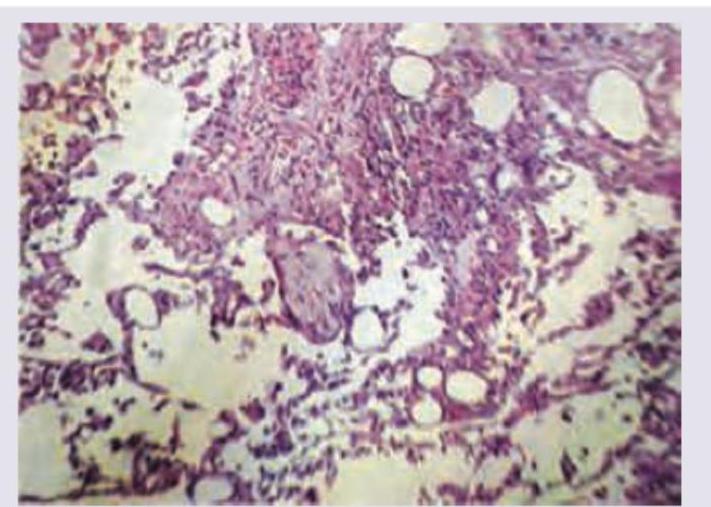
Question 1: A patient with a depressive illness is brought to casualty with acute breathlessness. X-ray shows diffuse infiltrates in right middle lobe and right lower lobe. The patient expired. The lung specimen on biopsy shows:
- A. Pulmonary alveolar proteinosis
- B. Tuberculosis
- C. Aspiration pneumonitis (Correct Answer)
- D. Fat embolism syndrome
Explanation: ***Aspiration pneumonitis*** - The lung biopsy shows **alveolar necrosis** and intra-alveolar edema with **foreign body giant cells** formed in response to aspirated material—these are the characteristic histologic features of aspiration pneumonitis. - The clinical context strongly supports this diagnosis: the patient's **depressive illness** predisposes to impaired consciousness or reflexes, increasing aspiration risk. The X-ray findings of diffuse infiltrates in the **right middle and lower lobes** are classic sites for aspirated contents due to anatomical positioning (right main bronchus is more vertical and wider). - Aspiration pneumonitis results from chemical injury to lung tissue from acidic gastric contents, causing acute inflammation, necrosis, and foreign body reaction. *Pulmonary alveolar proteinosis* - Characterized by accumulation of **lipid-rich proteinaceous material (surfactant)** in the alveoli, appearing as granular, eosinophilic debris on histology with PAS-positive staining—not alveolar necrosis with foreign body giant cells. - While it can cause diffuse infiltrates on X-ray and breathlessness, the histologic pattern is distinct, and there is no predisposing clinical context for aspiration. *Tuberculosis* - Typically shows **caseating granulomas** with epithelioid macrophages and Langhans giant cells on biopsy—these features are absent here. - TB usually has a more chronic presentation and different radiological pattern (upper lobe predominance, cavitation), not the acute presentation with aspiration risk factors seen in this case. *Fat embolism syndrome* - Would show **fat globules within pulmonary capillaries** and arterioles on histology (visible with Oil Red O or Sudan stains), along with pulmonary edema and hemorrhage—not foreign body giant cells and alveolar necrosis. - Typically occurs after long bone fractures or orthopedic trauma, which is not mentioned in this clinical scenario.
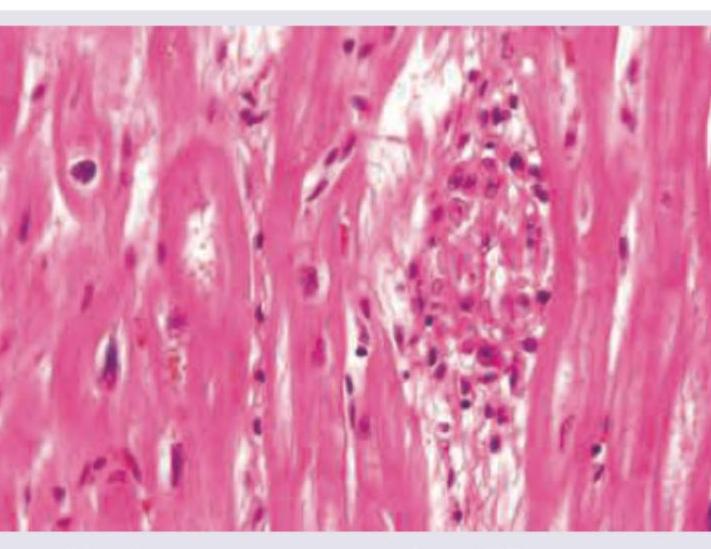
Question 2: An 18-year-old male with severe effort intolerance and dyspnea is found to have left atrial enlargement on Chest X-ray. Histopathological examination shows:
- A. Sarcoidosis
- B. TB
- C. Aschoff nodules (Correct Answer)
- D. Fungal granuloma
Explanation: ***Aschoff nodules*** - The clinical presentation of severe effort intolerance, dyspnea, and left atrial enlargement in an 18-year-old male is highly suggestive of **rheumatic heart disease**, a common cause of **mitral stenosis** leading to left atrial enlargement [1][2]. - **Aschoff nodules** are pathognomonic granulomatous lesions found in the myocardium during the acute phase of **rheumatic fever**, which can lead to rheumatic heart disease [1]. *Sarcoidosis* - While sarcoidosis can cause cardiac involvement (cardiomyopathy, arrhythmias), it typically presents with **non-caseating granulomas** and often affects other organs like lungs, skin, and eyes. - Cardiac sarcoidosis is less common in an 18-year-old and less likely to be the primary cause of isolated left atrial enlargement without other systemic features. *TB* - Tuberculosis can affect the pericardium (constrictive pericarditis) or myocardium, but it typically forms **caseating granulomas**. - Isolated left atrial enlargement due to TB is rare, and the clinical picture does not strongly suggest a tuberculous infection. *Fungal granuloma* - Fungal infections can cause granulomatous inflammation in the heart, especially in immunocompromised individuals. - However, the clinical presentation in an otherwise healthy 18-year-old is not typical for a fungal etiology, and fungal granulomas have distinct morphological features different from Aschoff bodies. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 566-567. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Cardiovascular Disease, pp. 293-294.
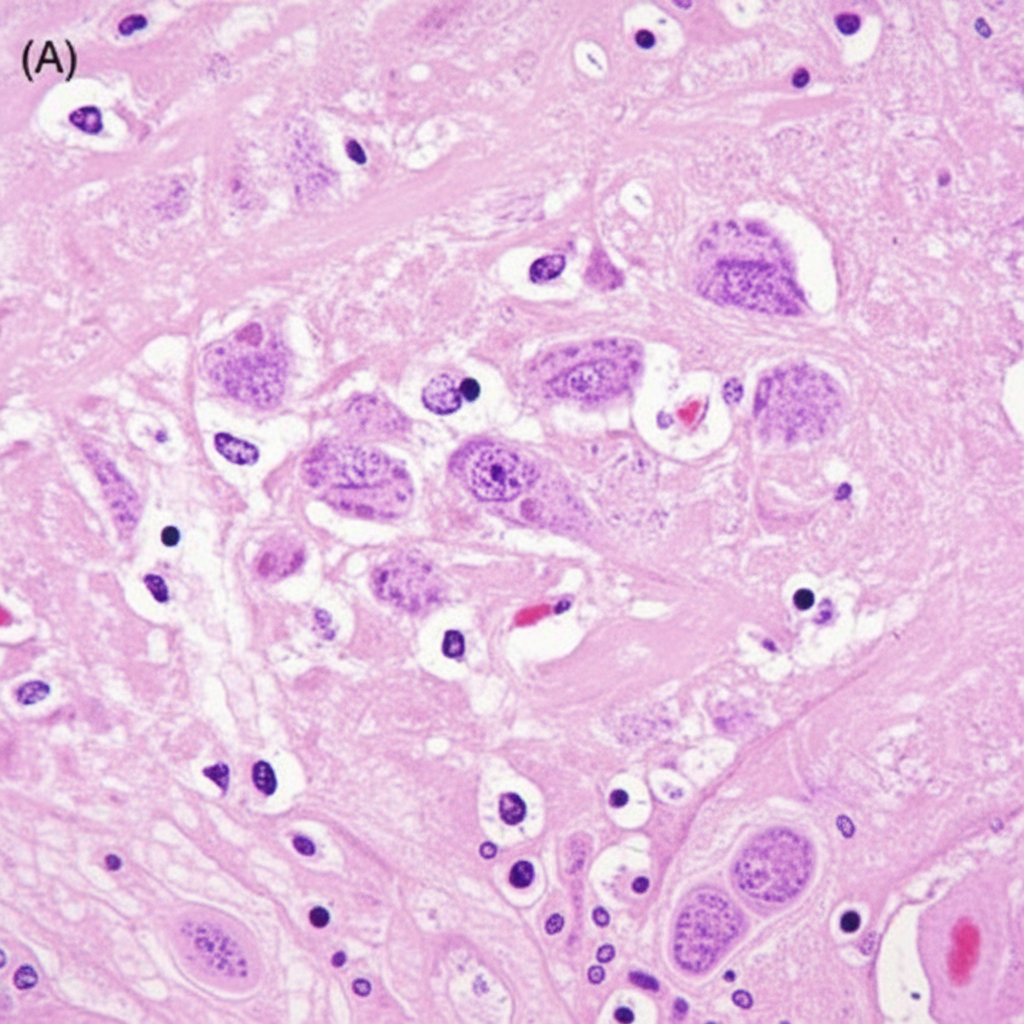
Question 3: The following brain biopsy of patient who presented with marked psychomotor agitation is diagnostic of?
- A. Rabies encephalitis (Correct Answer)
- B. Herpes simplex encephalitis
- C. Creutzfeldt-Jakob disease
- D. Japanese encephalitis
- E. Acute disseminated encephalomyelitis
Explanation: ***Correct: Rabies encephalitis*** - The brain biopsy showing **Negri bodies** (pathognomonic eosinophilic intracytoplasmic inclusions in pyramidal neurons of hippocampus and Purkinje cells of cerebellum) is diagnostic of **rabies encephalitis** - Clinical presentation of **marked psychomotor agitation** is characteristic of the furious form of rabies - Histopathology shows **perivascular lymphocytic cuffing** and neuronal degeneration along with Negri bodies - Rabies is caused by a **neurotropic RNA rhabdovirus** transmitted through animal bites *Incorrect: Herpes simplex encephalitis* - HSV encephalitis primarily affects the **temporal lobes** (hemorrhagic necrotizing encephalitis) - Histology shows **Cowdry type A intranuclear inclusions**, not cytoplasmic Negri bodies - Clinical features include fever, altered sensorium, and temporal lobe signs (olfactory/gustatory hallucinations) *Incorrect: Creutzfeldt-Jakob disease* - CJD is a **prion disease** showing **spongiform changes** (vacuolation) in the brain parenchyma - No viral inclusion bodies are seen - Clinical presentation includes rapidly progressive dementia, myoclonus, and ataxia *Incorrect: Japanese encephalitis* - JE causes **basal ganglia and thalamic involvement** (seen on neuroimaging) - Histology shows **neuronal necrosis and neuronophagia** but no characteristic inclusion bodies like Negri bodies - Clinical features include parkinsonian features and movement disorders *Incorrect: Acute disseminated encephalomyelitis* - ADEM is a **post-infectious demyelinating disease** showing perivenular demyelination - Histology shows demyelination with preservation of axons, not viral inclusions - Usually follows viral infection or vaccination
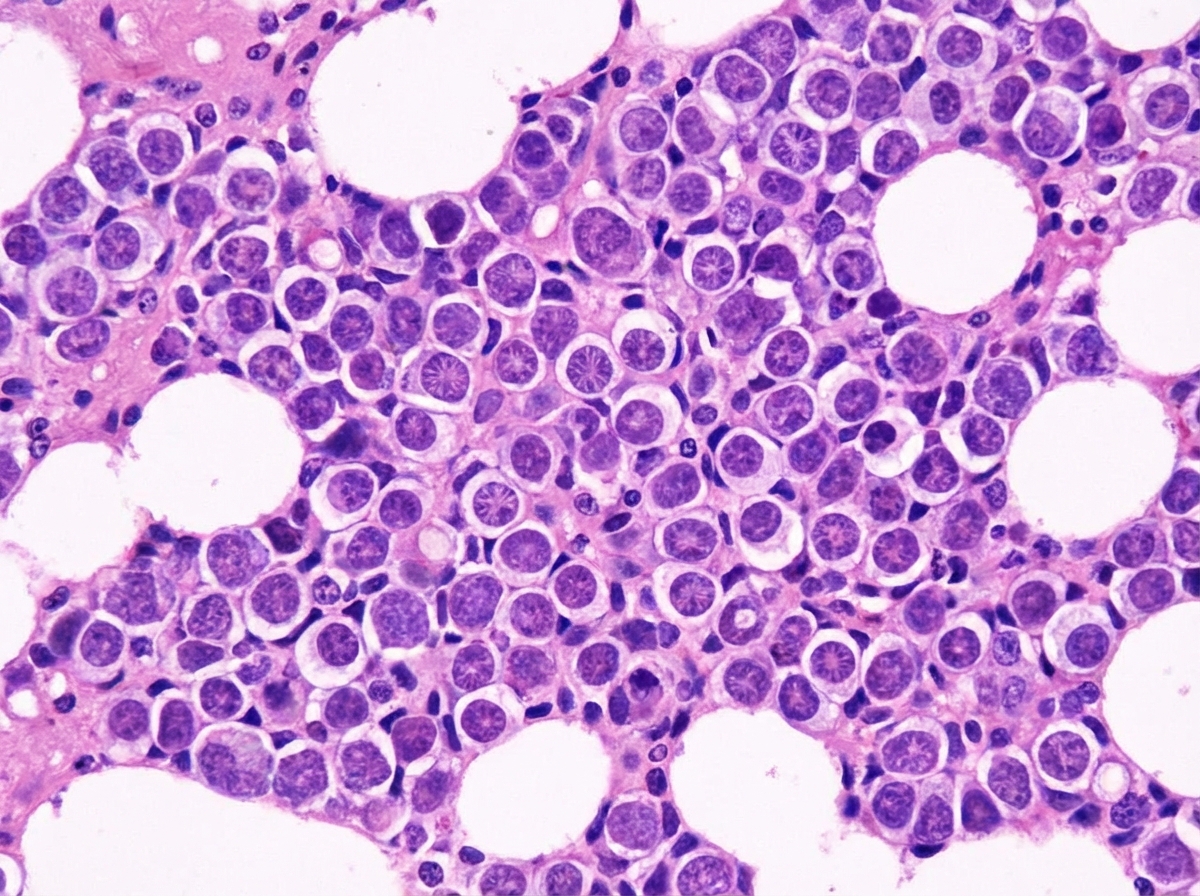
Question 4: A 70-year-old man presents with history of intractable diarrhea. His bone marrow and kidney biopsy are shown below. Which of the following is the most appropriate diagnosis?
- A. Leishmaniasis
- B. Multiple myeloma (Correct Answer)
- C. Lymphoma
- D. Urate nephropathy
- E. Amyloidosis
Explanation: ***Multiple myeloma*** - The combination of intractable diarrhea, bone marrow findings (likely showing **plasma cell proliferation**), and kidney biopsy findings (suggesting **cast nephropathy** or **amyloidosis**) is highly indicative of multiple myeloma [1][3][4]. - **Monoclonal immunoglobulin light chains** produced by plasma cells can cause renal damage and gastrointestinal symptoms like diarrhea [1][2][4]. *Leishmaniasis* - Characterized by **fever**, **splenomegaly**, and **pancytopenia**, with parasites found in macrophages. - While it can affect the bone marrow, it does not typically cause the specific kidney pathology or intractable diarrhea seen in this context. *Lymphoma* - Involves the proliferation of **lymphocytes** and can present with systemic symptoms like fever, weight loss, and lymphadenopathy. - While it can infiltrate the bone marrow and kidneys, it typically does not cause the specific renal casts or amyloid deposition seen in multiple myeloma, nor is intractable diarrhea a primary feature [5]. *Urate nephropathy* - Caused by the deposition of **uric acid crystals** in the renal tubules, leading to acute kidney injury, often in the context of tumor lysis syndrome or gout. - It does not explain the intractable diarrhea or the primary bone marrow pathology of plasma cell proliferation. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 616-617. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 607-608. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 617-618. [4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 618-619. [5] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 606-607.
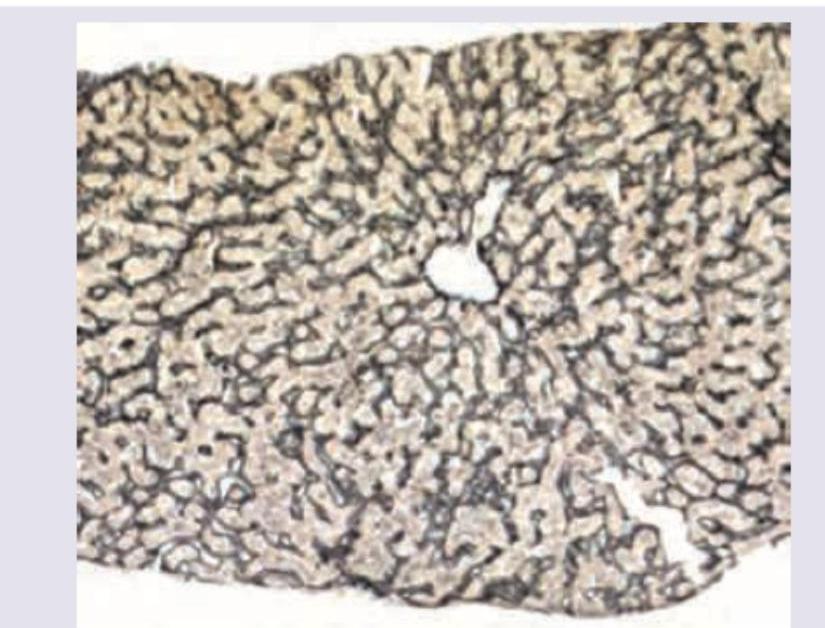
Question 5: Identify the stain shown in the liver section.
- A. Warthin starry
- B. Steiner silver stain
- C. Grimelius silver stain
- D. Gordon and Sweet's reticulin stain (Correct Answer)
Explanation: ***Gordon and Sweet's reticulin stain*** - The image shows **reticular fibers** in the liver, which appear as a delicate, branching network stained in **black**. This pattern is characteristic of a reticulin stain. - Reticulin stains are used to evaluate the **hepatic architecture** and detect its disruption in various liver diseases like cirrhosis. *Warthin starry* - The **Warthin-Starry stain** is primarily used to detect **spirochetes** (e.g., *Treponema pallidum* for syphilis) and certain bacteria like *Helicobacter pylori*. - It would show these organisms as black or brown, usually in a tissue section, but not the widespread network of reticular fibers seen here. *Steiner silver stain* - The **Steiner silver stain** is another type of silver impregnation stain used to detect **spirochetes** and other microorganisms, similar to Warthin-Starry. - It would not highlight the reticular fiber network of the liver in this specific pattern. *Grimelius silver stain* - The **Grimelius silver stain** is used to identify **neuroendocrine cells** and their granules, especially in tumors like carcinoids. - It stains the argyrophilic granules within these cells dark brown or black, which is distinct from the reticular network observed in the image.
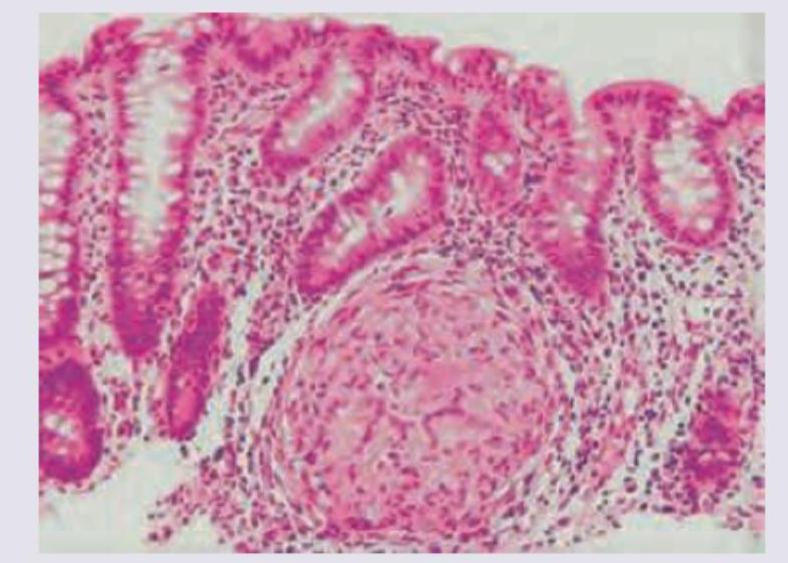
Question 6: A 50-year-old male presents with colicky abdominal pain and recurrent bloody diarrhea. Colonoscopy shows geographical ulcers. Histopathology is shown below. Diagnosis is:
- A. Pseudomembranous colitis
- B. Inflammatory bowel disease (Correct Answer)
- C. NHL
- D. Adenocarcinoma colon
Explanation: ***Inflammatory bowel disease*** - The presentation of **colicky abdominal pain**, **recurrent bloody diarrhea**, and **geographical ulcers** on colonoscopy are classic features of **Inflammatory Bowel Disease (IBD)**, specifically **Crohn's disease** [1]. - Histopathology in Crohn's disease often shows **transmural inflammation**, **non-caseating granulomas**, and **crypt abscesses**, which align with the clinical picture [1,2]. *Pseudomembranous colitis* - This condition is typically caused by **Clostridium difficile infection** and presents with watery diarrhea, fever, and abdominal pain, often after antibiotic use. - Colonoscopy reveals **yellowish-white plaques (pseudomembranes)**, not geographical ulcers. *NHL (Non-Hodgkin Lymphoma)* - While NHL can affect the colon, it usually presents with symptoms like **abdominal mass**, weight loss, and less commonly with recurrent bloody diarrhea as the primary symptom. - Colonoscopy findings would typically show a **mass lesion** or **polypoid growths**, not geographical ulcers. *Adenocarcinoma colon* - **Adenocarcinoma of the colon** is more common in older adults and typically presents with changes in bowel habits, rectal bleeding, and weight loss. - Colonoscopy would reveal a **polypoid mass** or an **ulcerative lesion** that is often solitary and malignant, not widespread geographical ulcers. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Alimentary System Disease, pp. 365-367. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 806-807.
About INI-CET 2017 Questions
This page contains 104 questions from the INI-CET 2017 paper, organised across 21 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the INI-CET exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your INI-CET goals.