INI-CET 2015 — Radiology
4 Previous Year Questions with Answers & Explanations
Identify the ECG given in the figure below.
A patient presents with neck pain and rigidity which gets relieved after bathing in hot water and exercise. Cervical X-ray is shown below. What is your diagnosis?

In the condition shown below, rib notching is present in which of the following ribs? (AIIMS Nov 2015)
What is the best diagnostic investigation for acute appendicitis in children?
INI-CET 2015 - Radiology INI-CET Practice Questions and MCQs
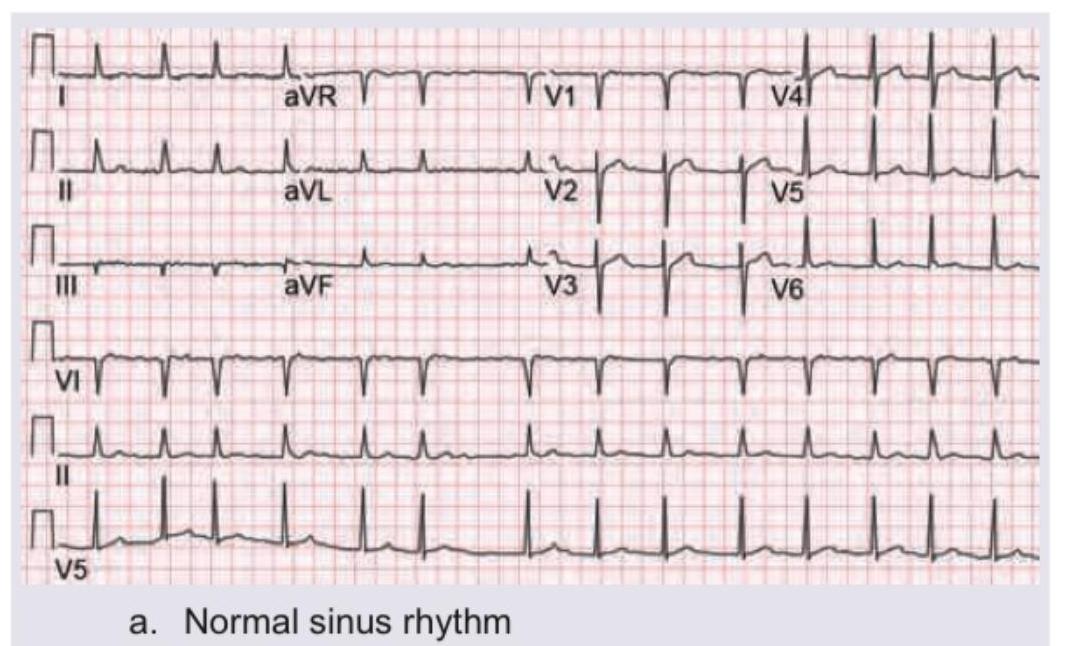
Question 1: Identify the ECG given in the figure below.
- A. Normal sinus rhythm (Correct Answer)
- B. Paroxysmal supraventricular tachycardia
- C. Atrial fibrillation
- D. Ventricular fibrillation
Explanation: ***Normal sinus rhythm*** - The ECG shows regular **P waves** followed by **QRS complexes**, with a consistent PR interval and a heart rate between 60-100 beats per minute, which are all characteristics of a normal sinus rhythm. - The QRS complexes are narrow, indicating normal ventricular depolarization, and the T waves are appropriately configured. *Paroxysmal supraventricular tachycardia* - This rhythm would typically show a **very rapid heart rate** (150-250 bpm) with narrow QRS complexes and often obscured or absent P waves. - The rate in this ECG is clearly within the normal range, and P waves are distinctly visible before each QRS. *Atrial fibrillation* - Atrial fibrillation is characterized by an **irregularly irregular rhythm**, absence of distinct P waves, and an erratic baseline due to chaotic atrial activity. - This ECG clearly shows a regular rhythm with discernible P waves. *Ventricular fibrillation* - Ventricular fibrillation is a life-threatening arrhythmia characterized by completely **chaotic and irregular electrical activity** in the ventricles, resulting in no identifiable P waves, QRS complexes, or T waves. - The ECG in the image shows clearly defined, organized waveforms, making ventricular fibrillation incorrect.
Question 2: A patient presents with neck pain and rigidity which gets relieved after bathing in hot water and exercise. Cervical X-ray is shown below. What is your diagnosis?
- A. Spondylolisthesis
- B. Spondylosis
- C. Spondylitis (Correct Answer)
- D. Spondyloptosis
Explanation: ***Spondylitis (Ankylosing Spondylitis)*** - The image shows **fusion of vertebral bodies** (ankylosis) and an appearance consistent with a **bamboo spine**, which is characteristic of advanced **Ankylosing Spondylitis**. - The clinical presentation is pathognomonic: **inflammatory back pain with morning stiffness** that is **relieved by activity and hot water bathing** (as opposed to mechanical pain which worsens with activity). - This is a classic presentation of inflammatory spondyloarthropathy, specifically ankylosing spondylitis. *Spondylolisthesis* - This condition involves the **slippage of one vertebra over another**, which is not the primary finding on this X-ray. - While spondylolisthesis can cause neck pain, it does **not typically present with diffuse vertebral fusion** as seen here, and the pain would worsen with activity (mechanical pattern), not improve. *Spondylosis* - Spondylosis refers to **degenerative changes** of the spine, often involving **osteophytes** and **disc space narrowing**. - While some degenerative changes may be present, the pronounced fusion and **"bamboo spine" appearance** go beyond typical spondylosis and indicate an inflammatory process. - Degenerative pain typically **worsens with activity**, unlike the relief with exercise seen in this patient. *Spondyloptosis* - Spondyloptosis is an **extreme form of spondylolisthesis** where one vertebra has completely slipped off the one below it (Grade V slip). - This severe displacement is not apparent on the X-ray; instead, there is **fusion rather than translational instability**.
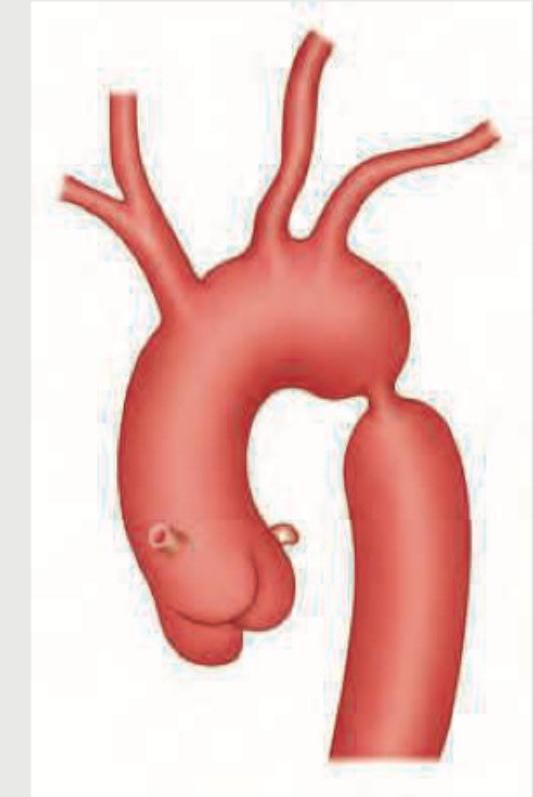
Question 3: In the condition shown below, rib notching is present in which of the following ribs? (AIIMS Nov 2015)
- A. 3rd to 9th ribs (Correct Answer)
- B. 1st to 9th ribs
- C. 11th and 12th ribs
- D. All ribs
Explanation: **3rd to 9th ribs** - The image provided depicts **coarctation of the aorta**, characterized by a narrowing of the aorta, typically distal to the origin of the left subclavian artery. - In coarctation of the aorta, collateral circulation develops through the **intercostal arteries** to bypass the constriction, leading to their enlargement and subsequent erosion of the inferior margins of the **3rd to 9th ribs**, a finding known as "rib notching." *1st to 9th ribs* - While rib notching affects upper ribs, it typically **spares the 1st and 2nd ribs** because the superior intercostal arteries (which supply these ribs) originate directly from the subclavian artery, often proximal to the coarctation, so they do not participate in collateral circulation as significantly. - The pattern of notching is usually more concentrated in the mid-thoracic region. *11th and 12th ribs* - Rib notching from coarctation of the aorta is rarely observed in the **floating ribs** (11th and 12th ribs). - These ribs have a different anatomical relationship with the pleura and typically do not bear the brunt of increased collateral flow from the intercostal arteries in the same way as the higher ribs. *All ribs* - Rib notching is a localized phenomenon reflecting increased blood flow through specific intercostal arteries involved in collateral circulation due to aortic coarctation. - Therefore, it does **not affect all ribs**, and its absence in certain ribs (like the 1st, 2nd, 11th, and 12th) helps differentiate this condition radiologically.
Question 4: What is the best diagnostic investigation for acute appendicitis in children?
- A. MRI
- B. CECT
- C. USG (Correct Answer)
- D. X-ray
Explanation: **Explanation:** The diagnosis of acute appendicitis in children relies on balancing diagnostic accuracy with the principles of radiation safety (**ALARA principle** – As Low As Reasonably Achievable). **Why USG is the Correct Answer:** Ultrasonography (USG) is the **initial and best diagnostic investigation** of choice in the pediatric population. Children have a thinner abdominal wall and less omental fat, which allows for better visualization of the appendix using a high-frequency linear transducer. It is non-invasive, widely available, and, most importantly, avoids exposure to ionizing radiation, to which the developing pediatric tissues are highly sensitive. * **Key USG finding:** A non-compressible, blind-ended tubular structure in the right iliac fossa with an outer diameter **>6 mm**. **Why Other Options are Incorrect:** * **CECT (Contrast-Enhanced CT):** While CECT is the **most sensitive and specific** (Gold Standard) investigation for appendicitis in adults, it is reserved as a second-line study in children if USG is inconclusive. This is due to the high radiation dose and potential risks of IV contrast. * **MRI:** MRI is highly accurate and avoids radiation, but it is not the "best" initial choice due to high cost, limited availability, and the frequent need for sedation in young children to ensure motion-free images. It is primarily used in pregnant patients. * **X-ray:** Plain radiographs have very low sensitivity. While they may occasionally show a radio-opaque **appendicolith** (fecalith) or localized ileus, they cannot definitively diagnose or rule out appendicitis. **Clinical Pearls for NEET-PG:** * **Target Sign:** Seen on axial USG/CT sections representing the inflamed layers of the appendix. * **McBurney’s Point:** Maximum tenderness located 1/3rd of the distance from the ASIS to the umbilicus. * **Alvarado Score:** A clinical scoring system used to risk-stratify patients; a score of ≥7 is highly suggestive of appendicitis.