INI-CET 2015 — Pharmacology
3 Previous Year Questions with Answers & Explanations
Methacholine acts primarily at which receptor?
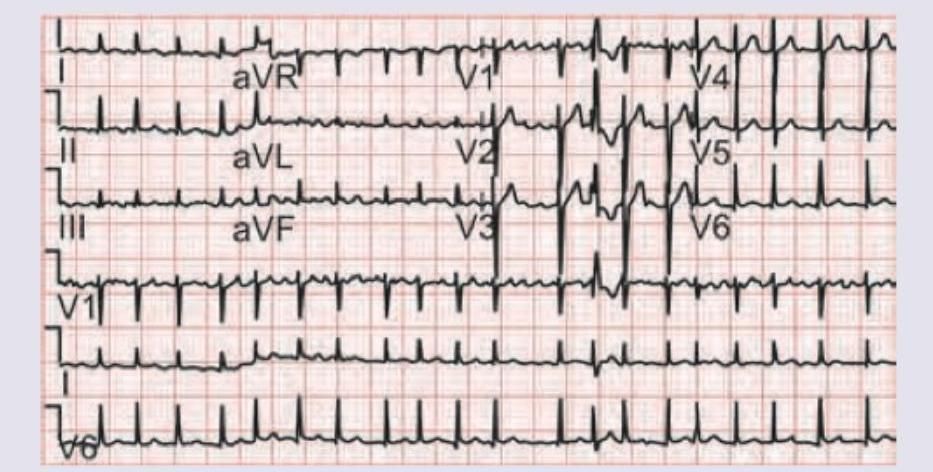
A 60-year-old hypertension patient presents with palpitations and pre-syncope. ECG was done. All drugs can be used for management of this condition except:
What is the drug of choice for pregnancy-induced hypertension?
INI-CET 2015 - Pharmacology INI-CET Practice Questions and MCQs
Question 1: Methacholine acts primarily at which receptor?
- A. M1
- B. M2
- C. M3 (Correct Answer)
- D. M4
Explanation: ***M3*** - **Methacholine** is a non-selective muscarinic agonist that acts at all muscarinic receptors, but its **primary clinically relevant effects**, particularly in the airways (e.g., bronchoconstriction in asthma challenge tests), are mediated through **M3 receptors**. - **M3 receptors** are Gq-coupled and lead to **smooth muscle contraction**, glandular secretion, and vasodilation via nitric oxide release. *M1* - **M1 receptors** are primarily found in the central nervous system and autonomic ganglia, playing a role in **neuronal excitation** and **autonomic transmission**. - While methacholine can activate M1 receptors, this is not its predominant site of action for clinical uses. *M2* - **M2 receptors** are found in the heart and are Gi-coupled, leading to a **decrease in heart rate** and contractility. - While methacholine acts on M2 receptors, its most notable effects (like bronchoconstriction) are not primarily mediated through M2. *M4* - **M4 receptors** are primarily located in the central nervous system, where they modulate neurotransmitter release and contribute to **motor control** and cognition. - Methacholine has some affinity for M4, but it is not the primary receptor responsible for its clinically relevant effects.
Question 2: A 60-year-old hypertension patient presents with palpitations and pre-syncope. ECG was done. All drugs can be used for management of this condition except:
- A. Diltiazem
- B. Esmolol
- C. Amiodarone
- D. Adenosine (Correct Answer)
Explanation: ***Adenosine*** - The ECG shows **atrial fibrillation with rapid ventricular response** and evidence of **pre-excitation** (short PR interval, delta wave), suggesting **Wolff-Parkinson-White (WPW) syndrome** complicated by atrial fibrillation. - Adenosine is **absolutely contraindicated** in AF with WPW syndrome because it causes profound AV nodal blockade, forcing all conduction down the accessory pathway, which can precipitate **life-threatening ventricular fibrillation**. - Among AV nodal blockers, **adenosine poses the greatest risk** due to its rapid, complete AV nodal blockade and is the classic teaching example of drugs to avoid in this condition. *Diltiazem* - **Calcium channel blockers** like diltiazem should generally be avoided in AF with WPW because they block the AV node and can worsen conduction via the accessory pathway, potentially leading to VF. - However, their effect is less abrupt than adenosine, making them somewhat less immediately dangerous. *Esmolol* - **Beta-blockers** like esmolol should also be avoided in AF with WPW syndrome because they block the AV node and can increase conduction through the accessory pathway. - Like calcium channel blockers, the risk is real but less catastrophic than with adenosine. *Amiodarone* - Amiodarone is a **Class III antiarrhythmic** that **can be safely used** for rhythm control in AF with WPW syndrome. - Unlike pure AV nodal blockers, it affects **both the AV node and accessory pathway**, helping to slow conduction through both routes without preferentially shunting impulses down the dangerous accessory pathway. - It is considered appropriate for pharmacological management of this condition.
Question 3: What is the drug of choice for pregnancy-induced hypertension?
- A. Atenolol
- B. Nitroprusside
- C. Enalapril
- D. Alpha-methyldopa (Correct Answer)
Explanation: **Explanation:** **Alpha-methyldopa** is the traditional drug of choice for chronic hypertension in pregnancy. It is a centrally acting alpha-2 adrenergic agonist that reduces sympathetic outflow. Its preference in pregnancy stems from its long-standing safety profile and the absence of long-term adverse effects on fetal development or neonatal hemodynamics. **Analysis of Options:** * **Atenolol (Option A):** Beta-blockers, particularly Atenolol, are generally avoided in early pregnancy as they are associated with **fetal growth restriction (IUGR)** and placental complications. * **Nitroprusside (Option B):** It is contraindicated in pregnancy (except in extreme emergencies) due to the risk of **fetal cyanide poisoning**. * **Enalapril (Option C):** ACE inhibitors and ARBs are strictly **contraindicated** in pregnancy. They are teratogenic and can cause fetal renal dysgenesis, oligohydramnios, and skull hypoplasia. **High-Yield Clinical Pearls for NEET-PG:** * **First-line agents:** While Methyldopa is the classic answer, current guidelines (like ACOG) also recommend **Labetalol** (often preferred for its faster onset) and **Nifedipine** (long-acting) as first-line options. * **Acute Hypertensive Crisis in Pregnancy:** The drugs of choice are **IV Labetalol** or **IV Hydralazine**. * **Preeclampsia Prophylaxis:** Low-dose **Aspirin** (started before 16 weeks) is used in high-risk patients. * **Magnesium Sulfate ($MgSO_4$):** This is the drug of choice for preventing and treating seizures in **Eclampsia**, not for blood pressure control.