INI-CET 2015 — Pediatrics
2 Previous Year Questions with Answers & Explanations
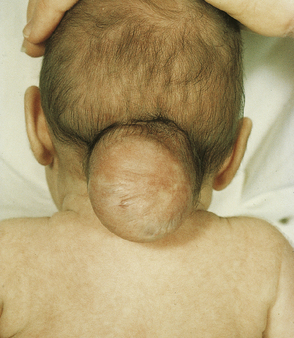
Identify the congenital defect seen in this baby.
A 4-year-old admitted in ward with pneumonia. He develops sudden onset of breathlessness. What is the next step in management?

INI-CET 2015 - Pediatrics INI-CET Practice Questions and MCQs
Question 1: Identify the congenital defect seen in this baby.
- A. Encephalocele (Correct Answer)
- B. Craniorachischisis totalis
- C. Cystic hygroma
- D. Cervical meningocele
Explanation: ***Encephalocele*** - A **neural tube defect** where brain tissue and/or meninges protrude through a **skull defect**, typically at the **occiput**, presenting as a cystic sac-like mass. - The image shows a characteristic **posterior cystic mass** protruding from the occipital region, which is pathognomonic for **occipital encephalocele**. *Craniorachischisis totalis* - The most severe **neural tube defect** with complete failure of neural tube closure involving both **cranial and spinal regions** along the entire length. - Would show extensive exposed **brain and spinal cord tissue** throughout the neural axis, not a localized occipital cystic mass. *Cystic hygroma* - A **lymphatic malformation** presenting as a multicystic, translucent mass typically in the **neck or axilla**. - Appears as **fluid-filled cystic structures** without neural tissue involvement and lacks the occipital location seen in this image. *Cervical meningocele* - A **localized spina bifida** where only **meninges** protrude through a cervical spine defect, forming a sac-like protrusion. - Limited to the **cervical/neck region** without cranial involvement, unlike the occipital location demonstrated here.
Question 2: A 4-year-old admitted in ward with pneumonia. He develops sudden onset of breathlessness. What is the next step in management?
- A. Intercostal drainage tube insertion
- B. Emergency needle thoracostomy (Correct Answer)
- C. Decrease mechanical ventilation setting
- D. Increase mechanical ventilation setting
Explanation: ***Emergency needle thoracostomy*** - This patient, a 4-year-old with pneumonia and sudden breathlessness, likely has a **tension pneumothorax**, which is a life-threatening emergency requiring immediate decompression. The chest X-ray shows a collapsed right lung and a mediastinal shift, consistent with tension pneumothorax. - An **emergency needle thoracostomy** (needle decompression) is the immediate life-saving procedure to relieve the pressure in a tension pneumothorax before more definitive treatment can be initiated. - Performed by inserting a large-bore needle (14-16G) into the **2nd intercostal space, mid-clavicular line** on the affected side. *Intercostal drainage tube insertion* - While an intercostal drainage tube (chest tube) is the definitive treatment for pneumothorax, it takes more time to insert and is not the immediate first step for a **tension pneumothorax** in an unstable patient. - The delay in performing needle decompression could be fatal in a rapidly deteriorating patient with tension pneumothorax. *Decrease mechanical ventilation setting* - Decreasing mechanical ventilation settings would not address the underlying pathology of a tension pneumothorax, which is trapped air causing lung collapse and mediastinal shift. - This action could further compromise the patient's respiratory status if the pneumothorax is severe and the patient is already hypoxemic. *Increase mechanical ventilation setting* - Increasing mechanical ventilation settings would likely worsen a **tension pneumothorax** by forcing more air into the pleural space and increasing intrathoracic pressure. - This would further compromise venous return to the heart and reduce cardiac output, rapidly leading to **cardiovascular collapse**.