Anesthesiology
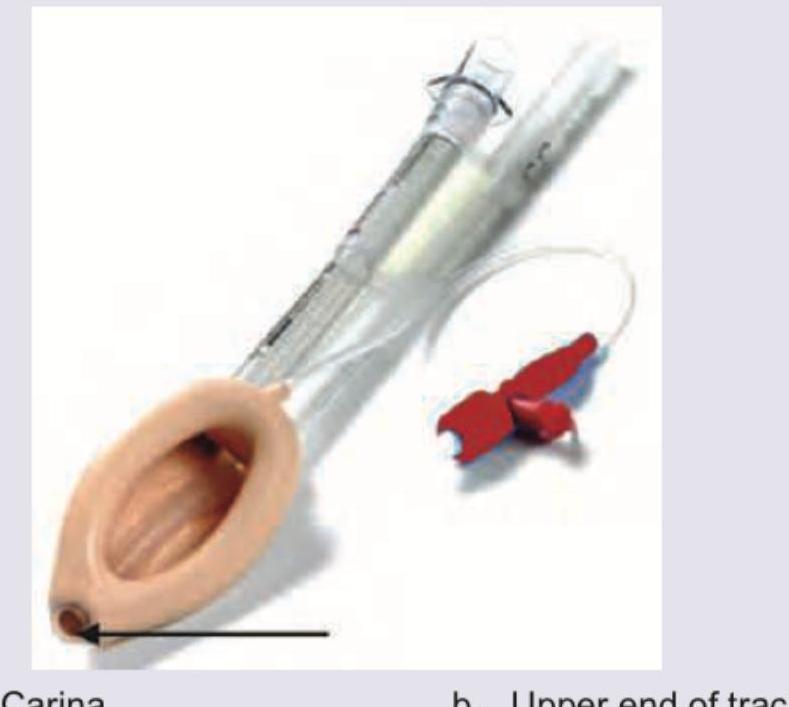
1 questionsThe diagram of a correctly positioned proseal-type Laryngeal Mask Airway is provided below. Above what site is the arrow marked area of the airway positioned?
INI-CET 2015 - Anesthesiology INI-CET Practice Questions and MCQs
Question 31: The diagram of a correctly positioned proseal-type Laryngeal Mask Airway is provided below. Above what site is the arrow marked area of the airway positioned?
- A. Carina
- B. Upper end of trachea
- C. Vocal cords (Correct Answer)
- D. Above esophagus
Explanation: ***Vocal cords*** - A correctly positioned laryngeal mask airway (LMA) forms a seal around the **laryngeal inlet**, with its tip resting in the **hypopharynx** superior to the esophagus. - The LMA cuff is designed to sit in the **piriform fossae**, sealing the entry to the esophagus, while the opening of the LMA tube is positioned over the **glottic opening**, which lies between the vocal cords. *Carina* - The **carina** is the bifurcation of the trachea into the main bronchi, which is much lower in the airway than where an LMA is designed to be positioned. - Positioning an LMA near the carina would mean it is deeply intubated into the trachea, which is not its intended use or design. *Upper end of trachea* - While the LMA provides an airway to the trachea, its cuff typically seals the laryngeal structures **above the trachea**, not within it. - The purpose of an LMA is to provide a supraglottic seal, meaning it sits above the true vocal cords and the tracheal opening. *Above esophagus* - Although the LMA's tip rests in the hypopharynx, providing a seal that prevents air from entering the esophagus, the primary target for airflow from the LMA is the **glottic opening (vocal cords)**, not simply "above the esophagus." - The device functions by sitting snugly over the laryngeal inlet, ensuring that ventilation is directed toward the trachea.
ENT
1 questionsThe most likely cause of persistent snoring and mouth breathing in a child is:
INI-CET 2015 - ENT INI-CET Practice Questions and MCQs
Question 31: The most likely cause of persistent snoring and mouth breathing in a child is:
- A. Tonsillar enlargement
- B. Adenoid enlargement (Correct Answer)
- C. Croup
- D. Paranasal sinus polyp
Explanation: ### Explanation **Correct Option: B. Adenoid Enlargement** The adenoids (nasopharyngeal tonsils) are located in the roof and posterior wall of the nasopharynx. In children, physiological hypertrophy occurs between ages 3 and 7. When pathologically enlarged, they obstruct the posterior choanae, leading to **obligate mouth breathing** and **snoring** due to vibration of the soft palate. This is the most common cause of pediatric nasal obstruction. Chronic obstruction leads to the characteristic "Adenoid Facies" (dull expression, open mouth, crowded teeth, and high-arched palate). **Analysis of Incorrect Options:** * **A. Tonsillar enlargement:** While palatine tonsil hypertrophy can cause snoring and Obstructive Sleep Apnea (OSA), it primarily affects the oropharynx. It is rarely the *sole* cause of persistent mouth breathing unless accompanied by adenoid hypertrophy. * **C. Croup (Laryngotracheobronchitis):** This is an acute inflammatory condition presenting with a "barking" cough, inspiratory stridor, and hoarseness. It is not a cause of chronic, persistent snoring or mouth breathing. * **D. Paranasal sinus polyp:** While polyps cause nasal obstruction, they are relatively rare in children. If present, they are often associated with Cystic Fibrosis or Kartagener’s syndrome. Adenoid hypertrophy is statistically far more common in the pediatric age group. **High-Yield Clinical Pearls for NEET-PG:** * **Investigation of Choice:** X-ray soft tissue nasopharynx (Lateral view) shows narrowing of the nasopharyngeal air space. * **Gold Standard Investigation:** Diagnostic nasal endoscopy. * **Associated Condition:** Adenoiditis often leads to **Eustachian tube dysfunction**, resulting in Otitis Media with Effusion (Glue Ear). * **Treatment:** Adenoidectomy is indicated if there is persistent mouth breathing, sleep apnea, or recurrent otitis media.
Obstetrics and Gynecology
1 questionsEarliest diagnosis of pregnancy can be established safely by?
INI-CET 2015 - Obstetrics and Gynecology INI-CET Practice Questions and MCQs
Question 31: Earliest diagnosis of pregnancy can be established safely by?
- A. USG for fetal cardiac activity
- B. Fetal cardiac Doppler study
- C. hCG levels (Correct Answer)
- D. MRI pelvis
Explanation: **Explanation:** The earliest biochemical marker for pregnancy is **human Chorionic Gonadotropin (hCG)**. It is produced by the syncytiotrophoblast cells following implantation. 1. **Why hCG levels are correct:** hCG can be detected in the maternal serum as early as **8–9 days after ovulation** (roughly 1 week before the missed period) using sensitive assays. In urine, it is typically detectable by the 4th week of gestation (around the time of the missed period). Since biochemical changes precede anatomical changes visible on imaging, hCG is the earliest safe method for diagnosis. 2. **Why other options are incorrect:** * **USG for fetal cardiac activity:** Transvaginal Sonography (TVS) can detect the gestational sac at 4.5–5 weeks, but fetal cardiac activity is only visible at **6–6.5 weeks**. This is significantly later than hCG detection. * **Fetal cardiac Doppler:** While Doppler can detect the fetal heart rate, it is generally used later than TVS (around 10–12 weeks via handheld Doppler) and is not the "earliest" diagnostic tool. * **MRI Pelvis:** MRI is highly accurate but is never used for the primary diagnosis of pregnancy due to high cost, lack of necessity, and the availability of simpler, faster tests. **High-Yield Clinical Pearls for NEET-PG:** * **Doubling Time:** In a healthy intrauterine pregnancy, serum β-hCG levels double every **48–72 hours** during the first trimester. * **Discriminatory Zone:** The level of hCG at which a gestational sac should be visible on TVS is **1,500–2,000 mIU/mL**. * **Peak Levels:** hCG levels reach their peak at **8–11 weeks** of gestation (approx. 100,000 mIU/mL) before declining to a plateau.
Pharmacology
1 questionsWhat is the drug of choice for pregnancy-induced hypertension?
INI-CET 2015 - Pharmacology INI-CET Practice Questions and MCQs
Question 31: What is the drug of choice for pregnancy-induced hypertension?
- A. Atenolol
- B. Nitroprusside
- C. Enalapril
- D. Alpha-methyldopa (Correct Answer)
Explanation: **Explanation:** **Alpha-methyldopa** is the traditional drug of choice for chronic hypertension in pregnancy. It is a centrally acting alpha-2 adrenergic agonist that reduces sympathetic outflow. Its preference in pregnancy stems from its long-standing safety profile and the absence of long-term adverse effects on fetal development or neonatal hemodynamics. **Analysis of Options:** * **Atenolol (Option A):** Beta-blockers, particularly Atenolol, are generally avoided in early pregnancy as they are associated with **fetal growth restriction (IUGR)** and placental complications. * **Nitroprusside (Option B):** It is contraindicated in pregnancy (except in extreme emergencies) due to the risk of **fetal cyanide poisoning**. * **Enalapril (Option C):** ACE inhibitors and ARBs are strictly **contraindicated** in pregnancy. They are teratogenic and can cause fetal renal dysgenesis, oligohydramnios, and skull hypoplasia. **High-Yield Clinical Pearls for NEET-PG:** * **First-line agents:** While Methyldopa is the classic answer, current guidelines (like ACOG) also recommend **Labetalol** (often preferred for its faster onset) and **Nifedipine** (long-acting) as first-line options. * **Acute Hypertensive Crisis in Pregnancy:** The drugs of choice are **IV Labetalol** or **IV Hydralazine**. * **Preeclampsia Prophylaxis:** Low-dose **Aspirin** (started before 16 weeks) is used in high-risk patients. * **Magnesium Sulfate ($MgSO_4$):** This is the drug of choice for preventing and treating seizures in **Eclampsia**, not for blood pressure control.
Radiology
1 questionsWhat is the best diagnostic investigation for acute appendicitis in children?
INI-CET 2015 - Radiology INI-CET Practice Questions and MCQs
Question 31: What is the best diagnostic investigation for acute appendicitis in children?
- A. MRI
- B. CECT
- C. USG (Correct Answer)
- D. X-ray
Explanation: **Explanation:** The diagnosis of acute appendicitis in children relies on balancing diagnostic accuracy with the principles of radiation safety (**ALARA principle** – As Low As Reasonably Achievable). **Why USG is the Correct Answer:** Ultrasonography (USG) is the **initial and best diagnostic investigation** of choice in the pediatric population. Children have a thinner abdominal wall and less omental fat, which allows for better visualization of the appendix using a high-frequency linear transducer. It is non-invasive, widely available, and, most importantly, avoids exposure to ionizing radiation, to which the developing pediatric tissues are highly sensitive. * **Key USG finding:** A non-compressible, blind-ended tubular structure in the right iliac fossa with an outer diameter **>6 mm**. **Why Other Options are Incorrect:** * **CECT (Contrast-Enhanced CT):** While CECT is the **most sensitive and specific** (Gold Standard) investigation for appendicitis in adults, it is reserved as a second-line study in children if USG is inconclusive. This is due to the high radiation dose and potential risks of IV contrast. * **MRI:** MRI is highly accurate and avoids radiation, but it is not the "best" initial choice due to high cost, limited availability, and the frequent need for sedation in young children to ensure motion-free images. It is primarily used in pregnant patients. * **X-ray:** Plain radiographs have very low sensitivity. While they may occasionally show a radio-opaque **appendicolith** (fecalith) or localized ileus, they cannot definitively diagnose or rule out appendicitis. **Clinical Pearls for NEET-PG:** * **Target Sign:** Seen on axial USG/CT sections representing the inflamed layers of the appendix. * **McBurney’s Point:** Maximum tenderness located 1/3rd of the distance from the ASIS to the umbilicus. * **Alvarado Score:** A clinical scoring system used to risk-stratify patients; a score of ≥7 is highly suggestive of appendicitis.
Surgery
1 questionsA patient underwent thyroidectomy for hyperthyroidism. Two days later, the patient presented with features of thyroid storm. What is the most likely cause?
INI-CET 2015 - Surgery INI-CET Practice Questions and MCQs
Question 31: A patient underwent thyroidectomy for hyperthyroidism. Two days later, the patient presented with features of thyroid storm. What is the most likely cause?
- A. Poor antibiotic coverage
- B. Rough handling during surgery
- C. Removal of parathyroid
- D. Inadequate preoperative preparation (Correct Answer)
Explanation: ### Explanation **1. Why "Inadequate Preoperative Preparation" is correct:** The primary goal of preoperative management in hyperthyroidism (especially Graves' disease) is to achieve a **euthyroid state** before surgery. If a patient is not properly prepared with antithyroid drugs (like Carbimazole or Methimazole) and Beta-blockers, the thyroid gland remains hyperactive. Surgical manipulation of an overactive gland triggers a massive release of stored thyroid hormones (T3 and T4) into the circulation. This sudden surge precipitates a **Thyroid Storm**, a life-threatening hypermetabolic state characterized by hyperpyrexia, tachycardia, and cardiac failure. **2. Why other options are incorrect:** * **Poor antibiotic coverage:** While this increases the risk of surgical site infection or sepsis, it does not directly trigger the hormonal surge characteristic of a thyroid storm. * **Rough handling during surgery:** While excessive manipulation can exacerbate hormone release, it rarely causes a storm if the patient was adequately prepared and euthyroid. Preparation is the definitive preventive factor. * **Removal of parathyroid:** This leads to **hypocalcemia** (tetany, Chvostek’s/Trousseau’s signs), not thyroid storm. **3. Clinical Pearls for NEET-PG:** * **Lugol’s Iodine:** Often given 10 days preoperatively to decrease the **vascularity** and friability of the gland (Plummer’s effect). * **Drug of choice for Thyroid Storm:** **Propylthiouracil (PTU)** is preferred over Methimazole because it also inhibits the peripheral conversion of T4 to T3. * **Beta-blockers (Propranolol):** Essential to control adrenergic symptoms and also help inhibit peripheral T4 to T3 conversion. * **Burch-Wartofsky Point Scale:** Used clinically to diagnose and grade the severity of a thyroid storm.