Anesthesiology
1 questionsWhat is the next best step in patient with the following capnography tracing?
INI-CET 2015 - Anesthesiology INI-CET Practice Questions and MCQs
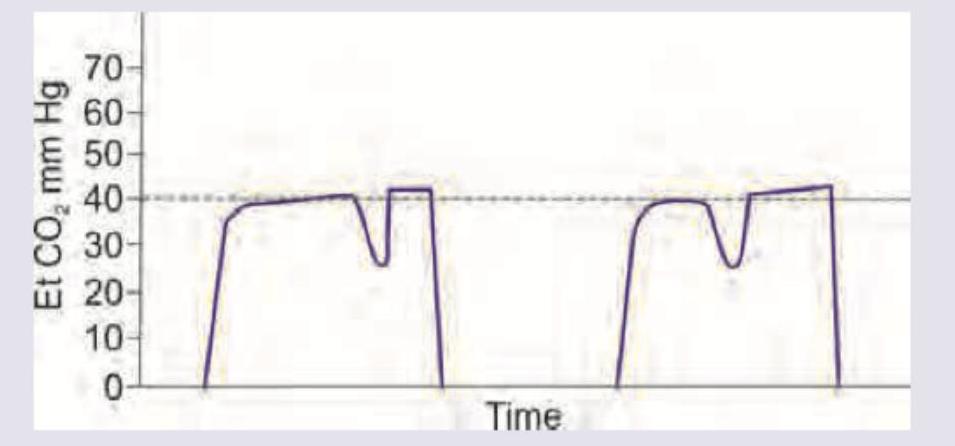
Question 21: What is the next best step in patient with the following capnography tracing?
- A. Check for position of endotracheal tube (Correct Answer)
- B. Check for connections of anesthesia machine
- C. Change the soda lime canister
- D. Give skeletal muscle relaxant
Explanation: ***Check for position of endotracheal tube*** - The "curare cleft" or re-curarization pattern on the capnography indicates that the patient is spontaneously breathing against the ventilator, suggesting the effects of **muscle relaxants are wearing off**. - This pattern can also indicate a partially obstructed or dislodged endotracheal tube, where the patient's spontaneous breaths against the obstruction cause a dip in the expiratory plateau. Therefore, checking the **endotracheal tube position** is a critical immediate step. *Check for connections of anesthesia machine* - While machine connections are important for proper ventilation, this specific **"curare cleft" pattern** is more indicative of patient respiratory effort or tube issues rather than a primary machine connection problem. - A machine connection issue would typically manifest as a **loss of waveform** or an abnormal overall shape, not specifically a dip in the expiratory plateau. *Change the soda lime canister* - A depleted soda lime canister causes an **elevation of the baseline** (inspire CO2 not zero) and a rise in end-tidal CO2, as CO2 is not effectively reabsorbed. - This capnography tracing does not show an elevated baseline, making a depleted soda lime canister an **unlikely cause** of the observed "curare cleft." *Give skeletal muscle relaxant* - While the "curare cleft" can indicate that the effects of muscle relaxants are waning and the patient is beginning to spontaneously breathe, the **immediate next step** is to ensure airway patency and security. - Administering a muscle relaxant without first checking the **airway and tube position** could mask a serious issue. Re-dosing relaxants might be considered after ensuring the airway is secure and the tube is correctly positioned if the patient's spontaneous breathing is detrimental.
Community Medicine
2 questionsThe following statistical diagram is called
The following statistical diagram is called
INI-CET 2015 - Community Medicine INI-CET Practice Questions and MCQs
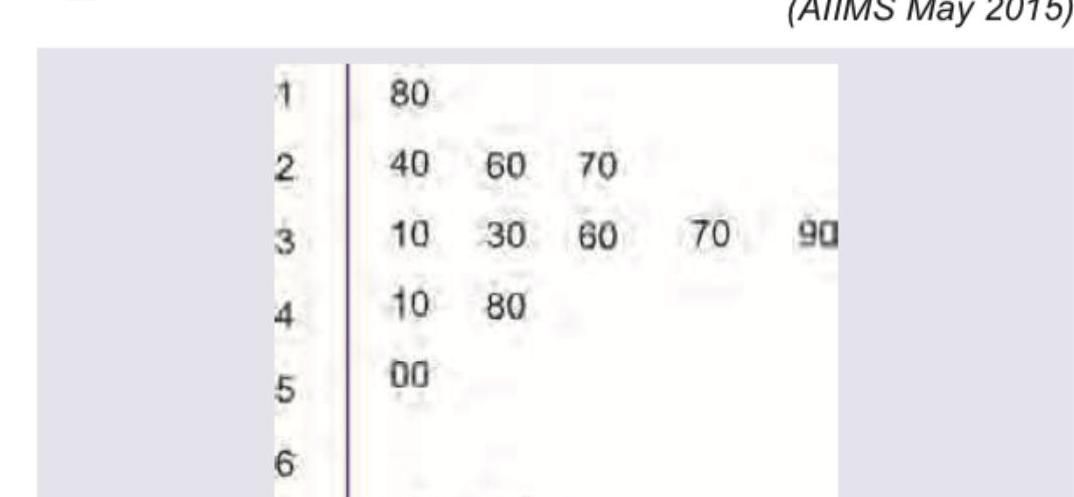
Question 21: The following statistical diagram is called
- A. Forest plot
- B. Funnel plot
- C. Box and whisker plot
- D. Stem and leaf plot (Correct Answer)
Explanation: ***Stem and leaf plot*** - This diagram displays quantitative data by separating each value into a "stem" (first digit(s)) and a "leaf" (last digit), arranged in order. - The provided image clearly shows digits on the left serving as stems (e.g., 1, 2, 3) and corresponding digits on the right as leaves (e.g., 80, 40, 60, 70), indicating a stem and leaf plot. *Forest plot* - A forest plot graphically presents the results of a **meta-analysis**, showing the estimated treatment effects and confidence intervals from multiple studies. - It does not organize individual data points by their numerical values in a stem-and-leaf structure. *Funnel plot* - A funnel plot is used to assess **publication bias** in a meta-analysis, plotting the effect size against a measure of study precision (e.g., standard error). - It appears as a scatter plot and does not resemble the structure of the given diagram. *Box and whisker plot* - A box and whisker plot displays the **five-number summary** of a set of data: minimum, first quartile, median, third quartile, and maximum. - It uses a rectangular "box" and "whiskers" extending from it, which is distinctly different from the digit-based organization seen in the image.
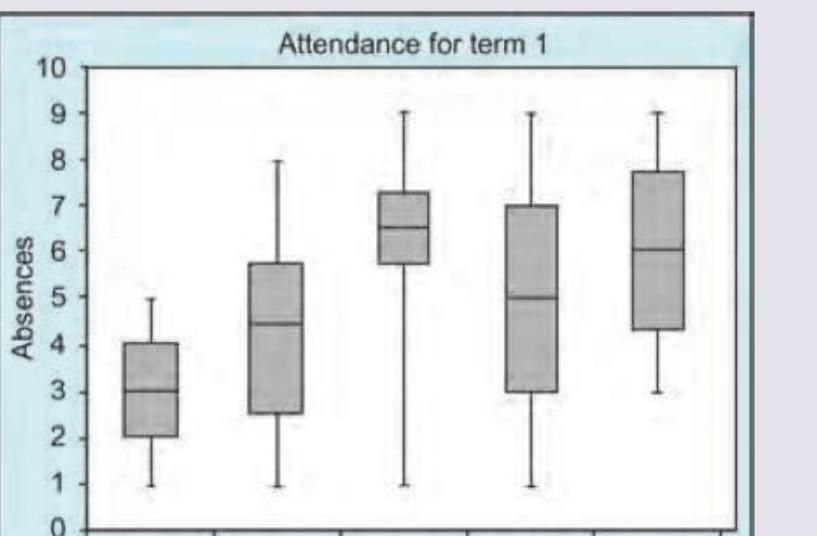
Question 22: The following statistical diagram is called
- A. Forest plot
- B. Funnel plot
- C. Box and whisker plot (Correct Answer)
- D. Stem and leaf plot
Explanation: ***Box and whisker plot*** - This diagram displays the **distribution** of a dataset through **quartiles**, with the "box" representing the interquartile range (25th to 75th percentile) and the "whiskers" extending to the minimum and maximum values (or a specified percentile range). - The horizontal line inside each box indicates the **median** of the data, providing a visual summary of central tendency and spread for different categories. *Forest plot* - A forest plot is typically used in **meta-analyses** to display the results of multiple studies measuring the same outcome. - It shows **individual study estimates** and their confidence intervals, along with an overall pooled estimate. *Funnel plot* - A funnel plot is used to assess **publication bias** in meta-analyses. - It plots the effect size against a measure of study precision, and in the absence of bias, the plot should resemble a symmetrical inverted funnel. *Stem and leaf plot* - A stem and leaf plot is a way of organizing numerical data to show its **distribution** while retaining the individual data points. - It separates each data point into a "stem" (the leading digit(s)) and a "leaf" (the trailing digit).
Forensic Medicine
1 questionsThe following image shows a victim of a firearm injury. What is the suspected distance of the shot?

INI-CET 2015 - Forensic Medicine INI-CET Practice Questions and MCQs
Question 21: The following image shows a victim of a firearm injury. What is the suspected distance of the shot?
- A. Close range
- B. Intermediate range (Correct Answer)
- C. Point blank range
- D. Distant shot
Explanation: ***Intermediate range*** - The image distinctly shows **stippling** (or tattooing), which consists of multiple small abrasions caused by **unburnt powder grains** impacting the skin. This pattern is characteristic of a shot fired from an intermediate range, typically 15 cm to 1 meter (6 inches to 3 feet). - The absence of a large **soot deposition** (fouling) and the presence of scattered powder grains confirm that the firearm was not fired at a very close or contact range. *Close range* - A close-range shot, usually within 10-15 cm (4-6 inches), would typically show **fouling** (blackening by soot) around the wound, in addition to minimal stippling. - The image does not display the extensive blackening or prominent soot deposition expected from a close-range shot. *Point blank range* - A point-blank (contact) shot implies the muzzle of the firearm was in direct contact with the skin, resulting in an **imprint of the muzzle** and significant **soot and gas forcefully driven into the wound track**. - Such shots often produce a stellate (star-shaped) wound due to gas expansion, and lack the widespread scattered stippling observed in the image because powder is deposited within the wound. *Distant shot* - A distant shot, typically beyond 1-1.5 meters (3-5 feet), would show **neither fouling nor stippling**. - Only the bullet perforates the skin, leaving a simple entrance wound without any surrounding marks from powder or gases.
Microbiology
4 questionsA 24-year-old female presented with an ulcer in the genital area. A giemsa stained cervical smear was prepared. Identify the causative agent: (AIIMS Nov 2015)
A 35-year-old male farmer presents with multiple discharging cervical sinuses. Which of these stains will be useful for the diagnosis and where does this organism normally colonize in the body? (AIIMS Nov 2015)
Stereotactic CT based aspiration from a patient with brain abscess was performed. Identify the organism seen and the stain used.
A patient presented with headache and projectile vomiting and altered sensorium. The following organism was demonstrated on India ink staining. What is the likely diagnosis?
INI-CET 2015 - Microbiology INI-CET Practice Questions and MCQs
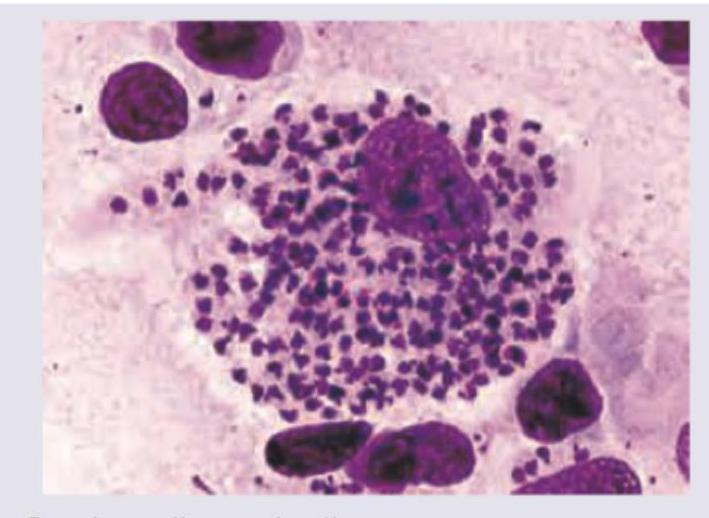
Question 21: A 24-year-old female presented with an ulcer in the genital area. A giemsa stained cervical smear was prepared. Identify the causative agent: (AIIMS Nov 2015)
- A. Gardnerella vaginalis
- B. Chlamydia
- C. Calymmatobacterium granulomatosis
- D. Haemophilus ducreyi (Correct Answer)
Explanation: ***Hemophilus ducreyi*** - The image shows numerous small, pleomorphic, gram-negative coccobacilli arranged in **'school of fish'** or parallel chains, characteristic of **_Haemophilus ducreyi_** on a Giemsa-stained smear. - This morphology, especially from a genital ulcer, is highly indicative of **chancroid**, caused by _H. ducreyi_. *Gardnerella vaginalis* - _Gardnerella vaginalis_ is associated with **bacterial vaginosis** and is characterized by the presence of **"clue cells"** (vaginal epithelial cells covered with coccobacilli) on microscopy. - It does not form the "school of fish" arrangement seen in the image, nor does it typically cause ulcerative lesions. *Chlamydia* - **_Chlamydia trachomatis_** causes various infections, including genital ulcers in cases of **lymphogranuloma venereum (LGV)**, but it is an obligate intracellular bacterium. - It would appear as **intracellular inclusions** on a Giemsa stain and would not show extracellular coccobacillary forms arranged in clusters as depicted. *Calymmatobacterium granulomatosis* - Previously known as _Calymmatobacterium granulomatosis_, now designated as **_Klebsiella granulomatis_**, this bacterium causes **granuloma inguinale (donovanosis)**, characterized by large, beefy-red ulcers. - Diagnostic features on Giemsa stain include **Donovan bodies** (intracellular bacilli within macrophages), which are not a prominent feature in the provided image.
Question 22: A 35-year-old male farmer presents with multiple discharging cervical sinuses. Which of these stains will be useful for the diagnosis and where does this organism normally colonize in the body? (AIIMS Nov 2015)
- A. Gram stain, hypopharynx
- B. PAS, intestine
- C. Modified kinyoun acid fast stain, mouth (Correct Answer)
- D. Grocott methenamine silver stain, vagina
Explanation: ***Modified Kinyoun acid-fast stain, mouth*** - This clinical presentation of **multiple discharging cervical sinuses** in a farmer is highly suggestive of **actinomycosis**, caused by *Actinomyces israelii*. - *Actinomyces israelii* is a **Gram-positive, non-spore-forming, anaerobic to microaerophilic rod** that is **partially acid-fast (modified Kinyoun acid-fast stain)** and a normal inhabitant of the **oral cavity, gastrointestinal tract, and female genital tract**. *Gram stain, hypopharynx* - While *Actinomyces israelii* would stain Gram-positive, the **Gram stain** alone is not specific enough to confirm actinomycosis, especially given the characteristic partially acid-fast nature. - The **hypopharynx** is not the primary or most common normal colonization site for *Actinomyces israelii*; the mouth is more accurate. *PAS, intestine* - The **Periodic Acid-Schiff (PAS) stain** is typically used to identify fungi, carbohydrates, and glycogen, not primarily *Actinomyces*. - While *Actinomyces* can be found in the intestine, it's not the most common colonization site associated with cervicofacial actinomycosis. *Grocott methenamine silver stain, vagina* - **Grocott Methenamine Silver (GMS) stain** is primarily used for the detection of fungi and some encapsulated bacteria, but not specifically *Actinomyces*. - Though *Actinomyces* can colonize the vagina, it's more commonly associated with pelvic actinomycosis, not the cervical presentation described.
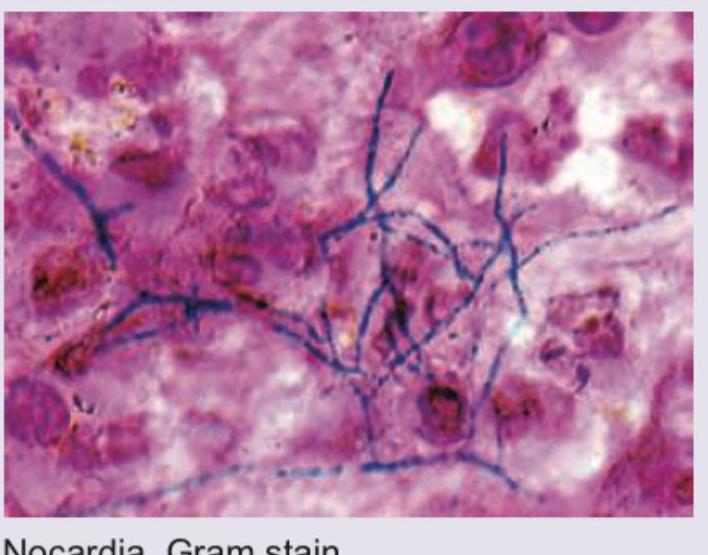
Question 23: Stereotactic CT based aspiration from a patient with brain abscess was performed. Identify the organism seen and the stain used.
- A. Nocardia, Gram stain (Correct Answer)
- B. Cryptococcus, India ink
- C. Streptococcus, Gram stain
- D. Staphylococcus, Gram stain
Explanation: ***Correct: Nocardia, Gram stain*** - The image displays **Gram-positive, branching filamentous bacteria**, which are characteristic morphological features of *Nocardia* species. These organisms are known to cause brain abscesses, especially in immunocompromised individuals. - The stain used is clearly a **Gram stain**, as evidenced by the purple/blue coloring of the bacterial cells (Gram-positive) against a pink/red background (counterstain). - *Nocardia* species are **weakly acid-fast** and show characteristic **branching, beaded filaments** that can be visualized with Gram staining. *Incorrect: Cryptococcus, India ink* - *Cryptococcus* is a **yeast** and would appear as round or oval budding cells, often with a prominent capsule, rather than branching filaments. - An **India ink stain** highlights the polysaccharide capsule of *Cryptococcus* as a clear halo against a black background, which is not what is seen in the image. *Incorrect: Streptococcus, Gram stain* - *Streptococcus* species are **Gram-positive cocci** that typically arrange in chains. They would appear as spherical cells in linear arrangements, not as filamentous structures. - While *Streptococcus* species can cause brain abscesses, their morphology in a Gram stain would be distinctly different from the branching filaments shown. *Incorrect: Staphylococcus, Gram stain* - *Staphylococcus* species are **Gram-positive cocci** that typically arrange in grape-like clusters. They would appear as spherical cells in irregular clumps, not as filamentous structures. - Similar to *Streptococcus*, their characteristic coccal morphology on a Gram stain would not match the filamentous structures observed in the image.
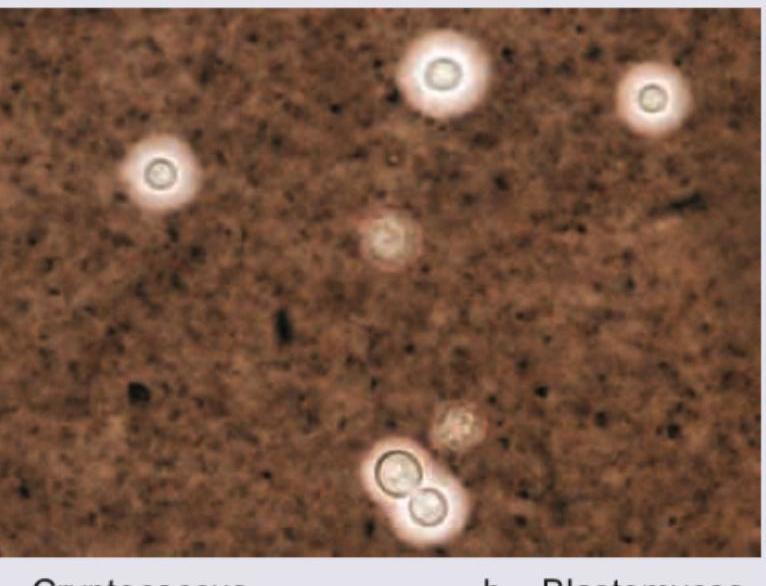
Question 24: A patient presented with headache and projectile vomiting and altered sensorium. The following organism was demonstrated on India ink staining. What is the likely diagnosis?
- A. Cryptococcus (Correct Answer)
- B. Blastomyces
- C. Histoplasma
- D. Coccidioides
Explanation: ***Cryptococcus*** - The image displays encapsulated yeast cells, characteristic of **_Cryptococcus neoformans_** or **_Cryptococcus gattii_**, which are commonly highlighted by **India ink staining** due to their large polysaccharide capsule. - The clinical presentation of headache, projectile vomiting, and altered sensorium strongly suggests **cryptococcal meningitis**, especially in immunocompromised individuals. *Blastomyces* - **_Blastomyces dermatitidis_** appears as large, broad-based budding yeast, which is distinct from the encapsulated yeasts seen in the image. - While it can cause CNS infection, its morphological characteristics under microscopy are different, and India ink is not its primary diagnostic stain. *Histoplasma* - **_Histoplasma capsulatum_** is a small, intracellular yeast, often seen within macrophages, and does not possess a prominent capsule that would be stained by India ink. - Neurological involvement is less common than with _Cryptococcus_ and the microscopic appearance is different. *Coccidioides* - **_Coccidioides immitis_** forms **spherules** containing **endospores** in tissue samples, a distinct morphology not seen in the provided image. - Although it can cause meningitis, its microscopic identification relies on finding these spherules, not encapsulated yeasts with India ink.
Obstetrics and Gynecology
1 questionsA 28 -year-old female patient presented with lower abdominal pain along with dysmenorrhea. The following finding was seen on laparoscopic examination. What is the likely diagnosis?

INI-CET 2015 - Obstetrics and Gynecology INI-CET Practice Questions and MCQs
Question 21: A 28 -year-old female patient presented with lower abdominal pain along with dysmenorrhea. The following finding was seen on laparoscopic examination. What is the likely diagnosis?
- A. Pelvic Endometriosis (Correct Answer)
- B. Pelvic Inflammatory Disease
- C. Ovarian Dermoid Cyst
- D. Adenomyosis
Explanation: ***Pelvic Endometriosis*** - The laparoscopic image shows classic findings of **endometriosis**, including **dark, hemorrhagic lesions** (powder-burn or gunshot lesions), adhesions, and potentially **endometriomas** (chocolate cysts) on the ovaries. - The patient's symptoms of **lower abdominal pain** and **dysmenorrhea** are highly characteristic of endometriosis, which involves the presence of endometrial-like tissue outside the uterus. - **Laparoscopy** is the gold standard for diagnosing endometriosis, revealing typical hemorrhagic implants and scarring. *Pelvic Inflammatory Disease* - PID typically presents with **acute pelvic pain**, **fever**, **purulent vaginal discharge**, and **cervical motion tenderness**. - Laparoscopic findings would show **hyperemia**, **purulent exudate**, and **tubo-ovarian abscesses**, not the dark hemorrhagic lesions seen here. - The chronic nature of dysmenorrhea and absence of infectious features make PID unlikely. *Ovarian Dermoid Cyst* - Dermoid cysts are **benign mature cystic teratomas** that appear as smooth, round cystic masses on laparoscopy. - They typically do not cause significant dysmenorrhea unless complicated by torsion or rupture. - The hemorrhagic implants and adhesions seen in the image are not consistent with dermoid cysts. *Adenomyosis* - Adenomyosis involves endometrial tissue within the **myometrium** (uterine muscle wall), causing an **enlarged, boggy uterus**. - Diagnosis is typically made by **ultrasound** or **MRI** showing thickened myometrium with heterogeneous echogenicity. - **Laparoscopy** would not reveal the characteristic dark hemorrhagic lesions seen in endometriosis, as adenomyosis is an intrauterine condition.
Pharmacology
1 questionsA 60-year-old hypertension patient presents with palpitations and pre-syncope. ECG was done. All drugs can be used for management of this condition except:
INI-CET 2015 - Pharmacology INI-CET Practice Questions and MCQs
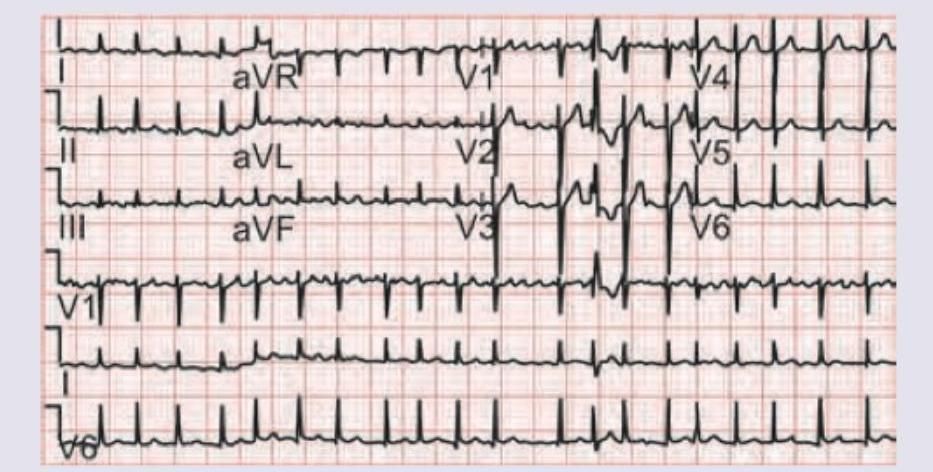
Question 21: A 60-year-old hypertension patient presents with palpitations and pre-syncope. ECG was done. All drugs can be used for management of this condition except:
- A. Diltiazem
- B. Esmolol
- C. Amiodarone
- D. Adenosine (Correct Answer)
Explanation: ***Adenosine*** - The ECG shows **atrial fibrillation with rapid ventricular response** and evidence of **pre-excitation** (short PR interval, delta wave), suggesting **Wolff-Parkinson-White (WPW) syndrome** complicated by atrial fibrillation. - Adenosine is **absolutely contraindicated** in AF with WPW syndrome because it causes profound AV nodal blockade, forcing all conduction down the accessory pathway, which can precipitate **life-threatening ventricular fibrillation**. - Among AV nodal blockers, **adenosine poses the greatest risk** due to its rapid, complete AV nodal blockade and is the classic teaching example of drugs to avoid in this condition. *Diltiazem* - **Calcium channel blockers** like diltiazem should generally be avoided in AF with WPW because they block the AV node and can worsen conduction via the accessory pathway, potentially leading to VF. - However, their effect is less abrupt than adenosine, making them somewhat less immediately dangerous. *Esmolol* - **Beta-blockers** like esmolol should also be avoided in AF with WPW syndrome because they block the AV node and can increase conduction through the accessory pathway. - Like calcium channel blockers, the risk is real but less catastrophic than with adenosine. *Amiodarone* - Amiodarone is a **Class III antiarrhythmic** that **can be safely used** for rhythm control in AF with WPW syndrome. - Unlike pure AV nodal blockers, it affects **both the AV node and accessory pathway**, helping to slow conduction through both routes without preferentially shunting impulses down the dangerous accessory pathway. - It is considered appropriate for pharmacological management of this condition.