All (36)Anesthesiology (2)Community Medicine (2)Dermatology (3)ENT (1)Forensic Medicine (1)Internal Medicine (3)Internal Medicine (1)Microbiology (5)Obstetrics and Gynecology (4)Pathology (3)Pathology (4)Pediatrics (2)Pharmacology (2)Radiology (2)Surgery (1)
Q11
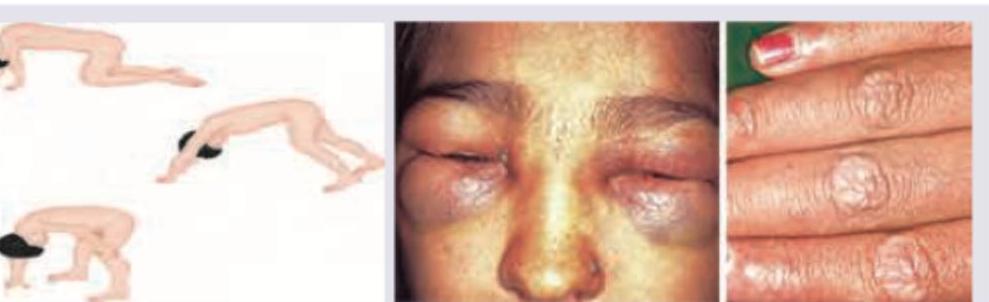
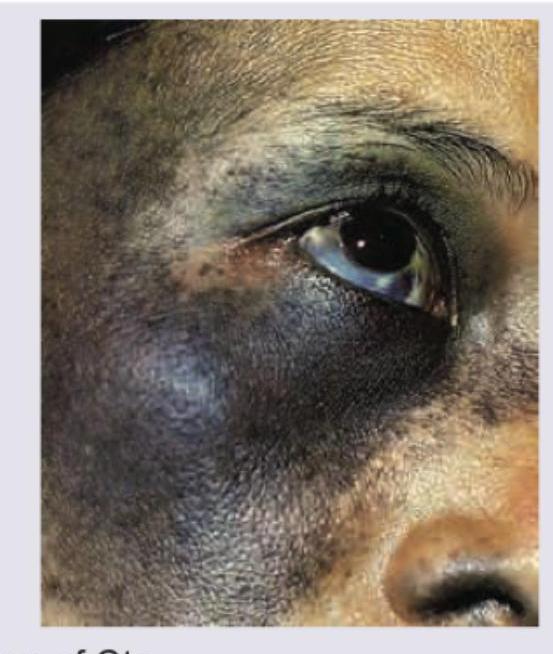
A 9-year-old girl presents with pigmentation over forehead and redness over upper eyelids. On physical examination following clinical sign was elicited. What is the next best step for diagnosis?
Q12
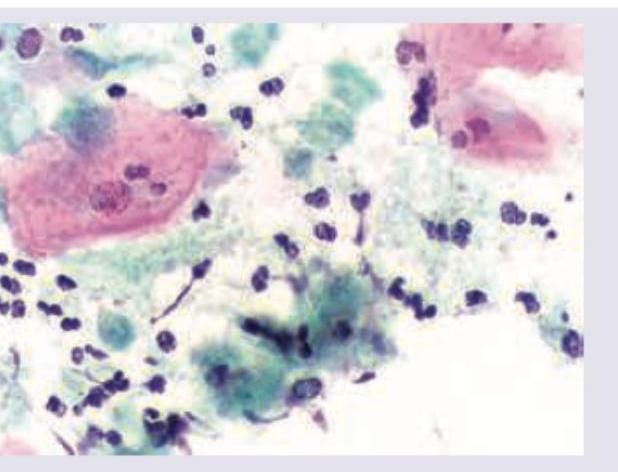
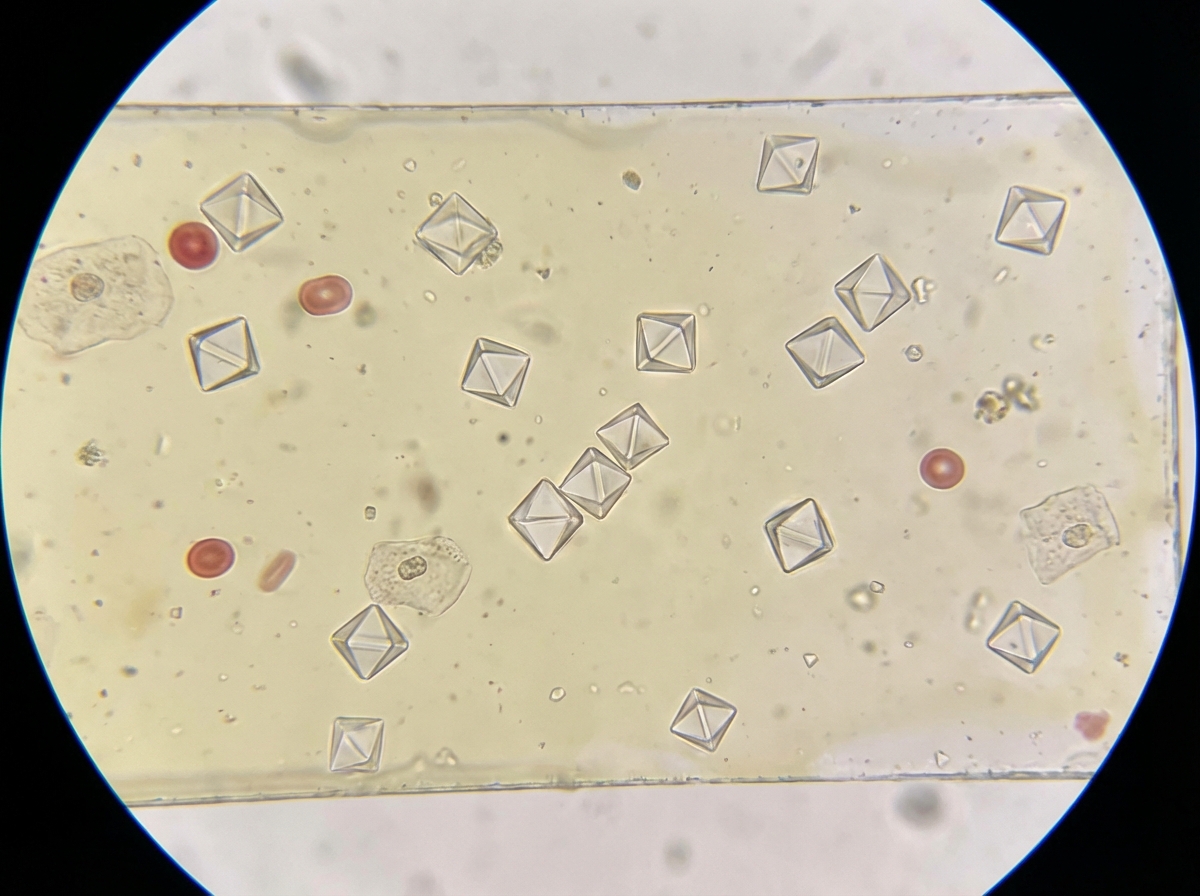
The image shows presence of:
Q13
An elderly patient presents with itchy tense blisters on normal looking skin as well as on urticarial plaques as shown below. The most probable diagnosis is: (AIIMS Nov 2015)