INI-CET 2015 — Obstetrics and Gynecology
4 Previous Year Questions with Answers & Explanations
The following CTG indicates:
The following CTG indicates:
A 28 -year-old female patient presented with lower abdominal pain along with dysmenorrhea. The following finding was seen on laparoscopic examination. What is the likely diagnosis?

Earliest diagnosis of pregnancy can be established safely by?
INI-CET 2015 - Obstetrics and Gynecology INI-CET Practice Questions and MCQs
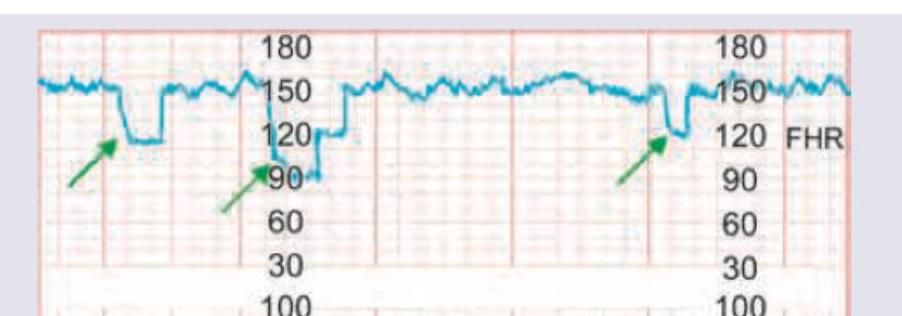
Question 1: The following CTG indicates:
- A. Early deceleration
- B. Late deceleration
- C. Variable deceleration (Correct Answer)
- D. Sinusoidal pattern
Explanation: ***Variable deceleration*** - This CTG shows **abrupt, irregular drops in fetal heart rate (FHR)** that do not consistently correspond to uterine contractions. The onset, depth, and duration of the decelerations vary, which is characteristic of variable decelerations. - Variable decelerations are often associated with **umbilical cord compression**, leading to a transient decrease in blood flow to the fetus. *Early deceleration* - Early decelerations are **gradual, symmetrical drops in FHR** that mirror the shape of the uterine contraction, meaning they begin and end with the contraction. - They are typically benign and caused by **fetal head compression** during contractions. *Late deceleration* - Late decelerations are **gradual, symmetrical drops in FHR** where the nadir of the deceleration occurs after the peak of the uterine contraction, and the recovery to baseline also occurs after the contraction has ended. - They are indicative of **uteroplacental insufficiency** and can be a sign of fetal hypoxia. *Sinusoidal pattern* - A sinusoidal pattern is characterized by a **smooth, undulating, sine wave-like FHR rhythm** with an amplitude of 5-15 bpm and a frequency of 2-5 cycles per minute, lasting for 20 minutes or more. - This pattern is highly concerning and is associated with **severe fetal anemia** or hypoxia.
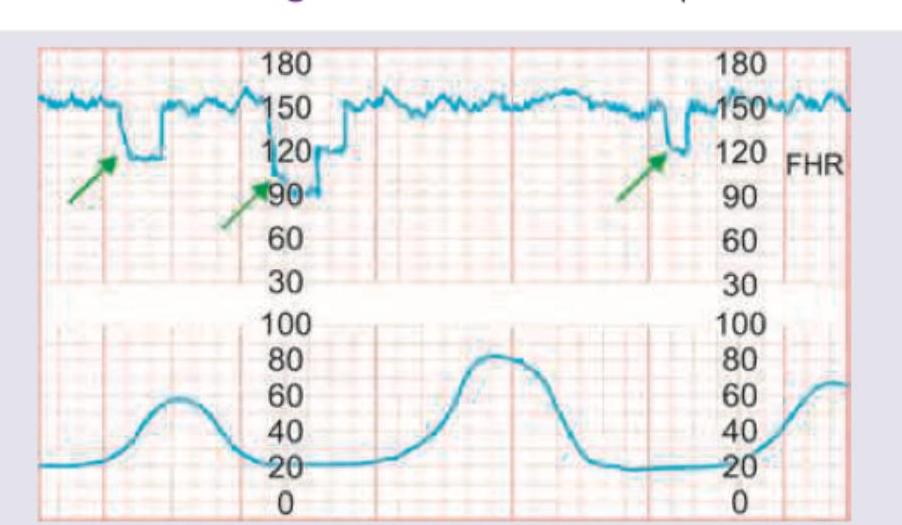
Question 2: The following CTG indicates:
- A. Fetal head compression (Correct Answer)
- B. Cord compression
- C. Normal tracing
- D. Fetal anemia
Explanation: ***Fetal head compression*** - The CTG shows **early decelerations**, characterized by a gradual decrease in fetal heart rate (FHR) that mirrors the contraction onset (as indicated by the green arrows and lower graph). - Early decelerations are typically benign and are caused by **fetal head compression**, which increases intracranial pressure and stimulates the vagus nerve. *Cord compression* - **Variable decelerations** are associated with cord compression and are characterized by an abrupt, jagged decrease in FHR that is variable in timing and shape relative to contractions. - The pattern displayed here is smooth and consistent with contractions, not the abrupt changes seen in variable decelerations. *Normal tracing* - A normal tracing would show a **baseline FHR within the normal range**, moderate variability, and either no decelerations or only occasional, reassuring accelerations. - The repeated decelerations observed here, while benign, indicate a physiological response to contractions and therefore do not represent a completely normal tracing. *Fetal anemia* - Fetal anemia can cause a variety of FHR patterns, including **tachycardia** (due to increased cardiac output) or **sinusoidal heart rate patterns**, which are smooth, undulating FHR tracings. - The decelerations seen in this CTG are not characteristic of fetal anemia.
Question 3: A 28 -year-old female patient presented with lower abdominal pain along with dysmenorrhea. The following finding was seen on laparoscopic examination. What is the likely diagnosis?
- A. Pelvic Endometriosis (Correct Answer)
- B. Pelvic Inflammatory Disease
- C. Ovarian Dermoid Cyst
- D. Adenomyosis
Explanation: ***Pelvic Endometriosis*** - The laparoscopic image shows classic findings of **endometriosis**, including **dark, hemorrhagic lesions** (powder-burn or gunshot lesions), adhesions, and potentially **endometriomas** (chocolate cysts) on the ovaries. - The patient's symptoms of **lower abdominal pain** and **dysmenorrhea** are highly characteristic of endometriosis, which involves the presence of endometrial-like tissue outside the uterus. - **Laparoscopy** is the gold standard for diagnosing endometriosis, revealing typical hemorrhagic implants and scarring. *Pelvic Inflammatory Disease* - PID typically presents with **acute pelvic pain**, **fever**, **purulent vaginal discharge**, and **cervical motion tenderness**. - Laparoscopic findings would show **hyperemia**, **purulent exudate**, and **tubo-ovarian abscesses**, not the dark hemorrhagic lesions seen here. - The chronic nature of dysmenorrhea and absence of infectious features make PID unlikely. *Ovarian Dermoid Cyst* - Dermoid cysts are **benign mature cystic teratomas** that appear as smooth, round cystic masses on laparoscopy. - They typically do not cause significant dysmenorrhea unless complicated by torsion or rupture. - The hemorrhagic implants and adhesions seen in the image are not consistent with dermoid cysts. *Adenomyosis* - Adenomyosis involves endometrial tissue within the **myometrium** (uterine muscle wall), causing an **enlarged, boggy uterus**. - Diagnosis is typically made by **ultrasound** or **MRI** showing thickened myometrium with heterogeneous echogenicity. - **Laparoscopy** would not reveal the characteristic dark hemorrhagic lesions seen in endometriosis, as adenomyosis is an intrauterine condition.
Question 4: Earliest diagnosis of pregnancy can be established safely by?
- A. USG for fetal cardiac activity
- B. Fetal cardiac Doppler study
- C. hCG levels (Correct Answer)
- D. MRI pelvis
Explanation: **Explanation:** The earliest biochemical marker for pregnancy is **human Chorionic Gonadotropin (hCG)**. It is produced by the syncytiotrophoblast cells following implantation. 1. **Why hCG levels are correct:** hCG can be detected in the maternal serum as early as **8–9 days after ovulation** (roughly 1 week before the missed period) using sensitive assays. In urine, it is typically detectable by the 4th week of gestation (around the time of the missed period). Since biochemical changes precede anatomical changes visible on imaging, hCG is the earliest safe method for diagnosis. 2. **Why other options are incorrect:** * **USG for fetal cardiac activity:** Transvaginal Sonography (TVS) can detect the gestational sac at 4.5–5 weeks, but fetal cardiac activity is only visible at **6–6.5 weeks**. This is significantly later than hCG detection. * **Fetal cardiac Doppler:** While Doppler can detect the fetal heart rate, it is generally used later than TVS (around 10–12 weeks via handheld Doppler) and is not the "earliest" diagnostic tool. * **MRI Pelvis:** MRI is highly accurate but is never used for the primary diagnosis of pregnancy due to high cost, lack of necessity, and the availability of simpler, faster tests. **High-Yield Clinical Pearls for NEET-PG:** * **Doubling Time:** In a healthy intrauterine pregnancy, serum β-hCG levels double every **48–72 hours** during the first trimester. * **Discriminatory Zone:** The level of hCG at which a gestational sac should be visible on TVS is **1,500–2,000 mIU/mL**. * **Peak Levels:** hCG levels reach their peak at **8–11 weeks** of gestation (approx. 100,000 mIU/mL) before declining to a plateau.