INI-CET 2015 — Dermatology
2 Previous Year Questions with Answers & Explanations
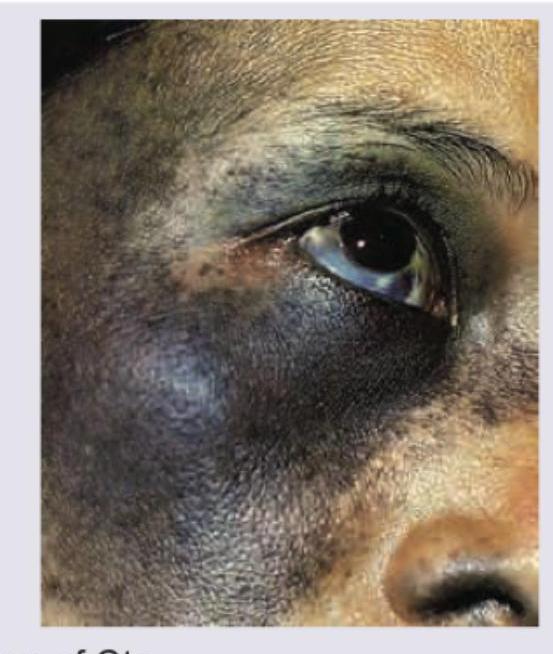
The image shows presence of:
An elderly patient presents with itchy tense blisters on normal looking skin as well as on urticarial plaques as shown below. The most probable diagnosis is: (AIIMS Nov 2015)

INI-CET 2015 - Dermatology INI-CET Practice Questions and MCQs
Question 1: The image shows presence of:
- A. Nevus of Ota (Correct Answer)
- B. Nevus spilus
- C. Giant melanocytic nevus of face
- D. Port wine stain
Explanation: - ***Nevus of Ota*** - The image exhibits a characteristic **blue-grey or brownish discoloration** on the face, specifically around the eye (periorbital region) and extending to the temple and cheek. - The presence of **scleral pigmentation** (blue discoloration of the sclera) is a classic finding associated with Nevus of Ota, due to dermal melanocytosis affecting both skin and ocular structures. - *Nevus spilus* - This condition presents as a **light brown patch** with speckles of darker macules or papules within it, resembling "spots on a spot." - It does not typically involve the deep blue-grey coloration or ocular pigmentation seen in the image. - *Giant melanocytic nevus of face* - While also a melanocytic nevus, a giant congenital melanocytic nevus is typically much larger, often covering extensive body areas, and has a more **uniform dark brown to black coloration** with a rugose or hairy surface, differing from the blue-grey hue and distribution shown. - Though it can occur on the face, the overall appearance, particularly the distinct blue-grey color and scleral involvement, is not typical for a giant melanocytic nevus. - *Port wine stain* - A port wine stain is a type of **capillary malformation** characterized by a flat, pink to red vascular lesion that darkens with age to a deep purple. - It blanches under pressure and is due to dilated capillaries, not melanin deposition, and does not cause the blue-grey pigmentation or scleral involvement seen here.
Question 2: An elderly patient presents with itchy tense blisters on normal looking skin as well as on urticarial plaques as shown below. The most probable diagnosis is: (AIIMS Nov 2015)
- A. Pemphigus vulgaris
- B. Linear IgA disease
- C. Bullous pemphigoid (Correct Answer)
- D. Dermatitis herpetiformis
Explanation: ***Bullous pemphigoid*** - This condition typically presents in **elderly patients** with **itchy, tense blisters** on either normal or erythematous/urticarial skin, which aligns with the clinical description and image. - The blisters in bullous pemphigoid are characterized by **subepidermal blistering**, meaning the epidermis separates from the dermis, resulting in tense, fluid-filled lesions. *Pemphigus vulgaris* - Characterized by **flaccid blisters** that rupture easily, leading to erosions, unlike the tense blisters seen in the image. - Pemphigus vulgaris frequently involves **mucous membranes** and is caused by autoantibodies against desmoglein 1 and 3, leading to intraepidermal blistering (acantholysis). *Linear IgA disease* - This autoimmune blistering condition typically presents with **annular or rosette-shaped lesions** with small peripheral blisters, often referred to as a "string of pearls" appearance, which is not evident in the image. - On **direct immunofluorescence**, it shows a linear deposition of IgA at the dermoepidermal junction. *Dermatitis herpetiformis* - Often presents with **intensely pruritic papules and vesicles** typically found on extensor surfaces (elbows, knees, buttocks), and the lesions are often excoriated due to scratching. - Strongly associated with **celiac disease** and characterized by granular IgA deposits in the dermal papillae on direct immunofluorescence, distinguishing it from the tense blisters seen.