INI-CET 2015
36 Previous Year Questions with Answers & Explanations
Internal Medicine
1 questionsIn the ECG shown below, which drug will not be given?
INI-CET 2015 - Internal Medicine INI-CET Practice Questions and MCQs
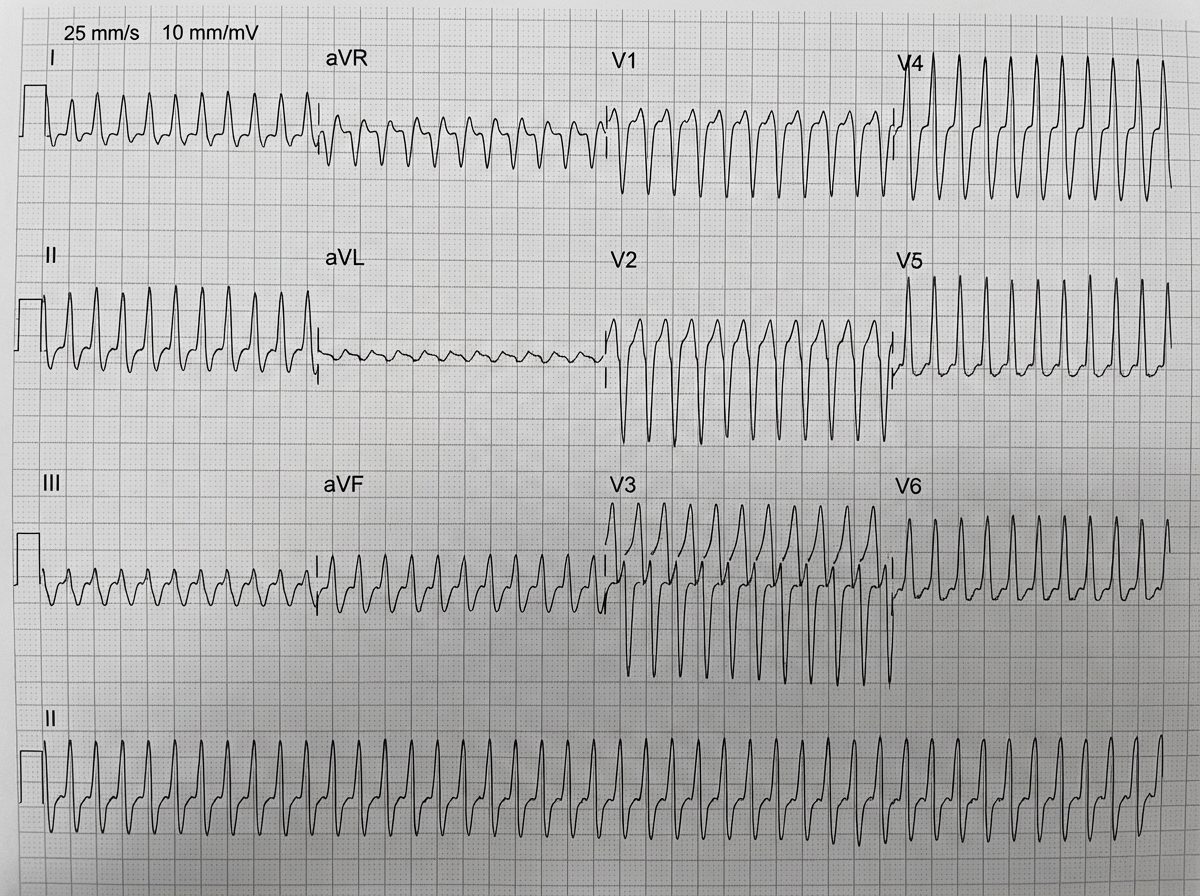
Question 1: In the ECG shown below, which drug will not be given?
- A. Adenosine (Correct Answer)
- B. Verapamil
- C. Diltiazem
- D. Flecainide
- E. Amiodarone
Explanation: ***Adenosine*** - The ECG shows a **wide complex tachycardia** with a regular rhythm and a rate of approximately 150 bpm. Given the wide QRS, the differential includes **ventricular tachycardia (VT)** or a **supraventricular tachycardia (SVT) with aberrancy**. - In wide complex tachycardia, **Adenosine** is contraindicated if there is suspicion of **ventricular tachycardia (VT)**, as it can cause **hemodynamic collapse** or **degenerate into ventricular fibrillation**. - Adenosine is primarily used for **narrow complex SVT** and should be avoided in wide complex tachycardias when VT cannot be excluded. *Verapamil* - Verapamil, a **calcium channel blocker**, can be used to slow the ventricular response in certain SVTs, but it is generally **contraindicated** in **wide complex tachycardias** of unknown origin because it can worsen hypotension or cause cardiovascular collapse if the rhythm is VT. - Its use in pre-excited atrial fibrillation can lead to **ventricular fibrillation**. *Diltiazem* - Diltiazem is a **non-dihydropyridine calcium channel blocker** similar to Verapamil. - It works by slowing conduction through the **AV node** and is effective for rate control in SVTs. However, it is also generally **contraindicated** in wide complex tachycardias if the origin is uncertain, particularly if **VT** is suspected, due to the risk of further **hemodynamic compromise**. *Flecainide* - Flecainide is a **Class IC antiarrhythmic drug** that prolongs the QRS duration. - It is typically used for the treatment of **supraventricular arrhythmias** and **ventricular arrhythmias** in patients without structural heart disease. However, it is **contraindicated** in patients with **structural heart disease** (e.g., myocardial infarction, heart failure) due to an increased risk of proarrhythmia and mortality. The ECG shows signs of an evolving MI or prior MI in the inferior leads, making flecainide a risky choice for this patient. *Amiodarone* - Amiodarone is a **Class III antiarrhythmic drug** that can be used for both **SVT with aberrancy** and **ventricular tachycardia**. - It is considered a **safe option** in wide complex tachycardia of uncertain etiology, as it is effective for both VT and SVT, and has a lower risk of causing hemodynamic collapse compared to other agents. - Amiodarone is often the preferred drug when the origin of wide complex tachycardia is unclear.
Pathology
5 questionsIn a patient, Mitral valve vegetations are seen along the lines of closure along with fusion of commissures. What is the likely diagnosis?

A 55-year-old male patient presented with a 4 month history of cough and hemoptysis. Bronchoscopy revealed an intrabronchial polyp. Biopsy from the polyp showed small cells with salt and pepper chromatin, with microscopic necrosis and 5 mitotic figures per 10 high power fields as shown below. Chromogranin staining was positive. What is the diagnosis and grade of the lesion?
Agarose gel electrophoresis from DNA of a population of cells as seen under ultraviolet light is shown below. What is the correct explanation for the finding seen in the band labeled as "C"?
The following is the FITC for IgG stained kidney specimen. What is this suggestive of?
The following microscopic appearance is that of a schwannoma which most commonly involves the cerebellopontine angle. What does the area marked with the arrow represent?
INI-CET 2015 - Pathology INI-CET Practice Questions and MCQs
Question 1: In a patient, Mitral valve vegetations are seen along the lines of closure along with fusion of commissures. What is the likely diagnosis?
- A. Libman-Sacks endocarditis
- B. Marantic endocarditis
- C. Bacterial endocarditis
- D. Rheumatic endocarditis (Correct Answer)
Explanation: ***Rheumatic endocarditis*** - **Rheumatic fever** is a common cause of **mitral valve disease**, leading to **vegetations along the lines of closure** [2] and characteristic **fusion of commissures** [1]. - This chronic inflammation results in **fibrosis** and **calcification**, causing **mitral stenosis** [3] or regurgitation. *Libman-Sacks endocarditis* - Characterized by **sterile vegetations** typically found on **both sides of the valve leaflets** (atrial and ventricular surfaces) [2], often associated with **Systemic Lupus Erythematosus (SLE)**. - It does not typically cause **commissural fusion** or significant valvular stenosis. *Marantic endocarditis* - Also known as **nonbacterial thrombotic endocarditis (NBTE)**, it involves **sterile vegetations** composed of fibrin and platelets, usually found on the **lines of closure** [2]. - It is associated with **debilitating illnesses** like cancer or sepsis, but **does not cause commissural fusion**. *Bacterial endocarditis* - Involves **large, destructive vegetations** that can be found on any part of the valve [2], often associated with **valve destruction**, **abscess formation**, and **septic emboli**. - While it causes vegetations, it typically **does not lead to commissural fusion** as a primary feature; fusion is more characteristic of chronic rheumatic heart disease. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 566-567. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, p. 568. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Cardiovascular Disease, pp. 293-294.
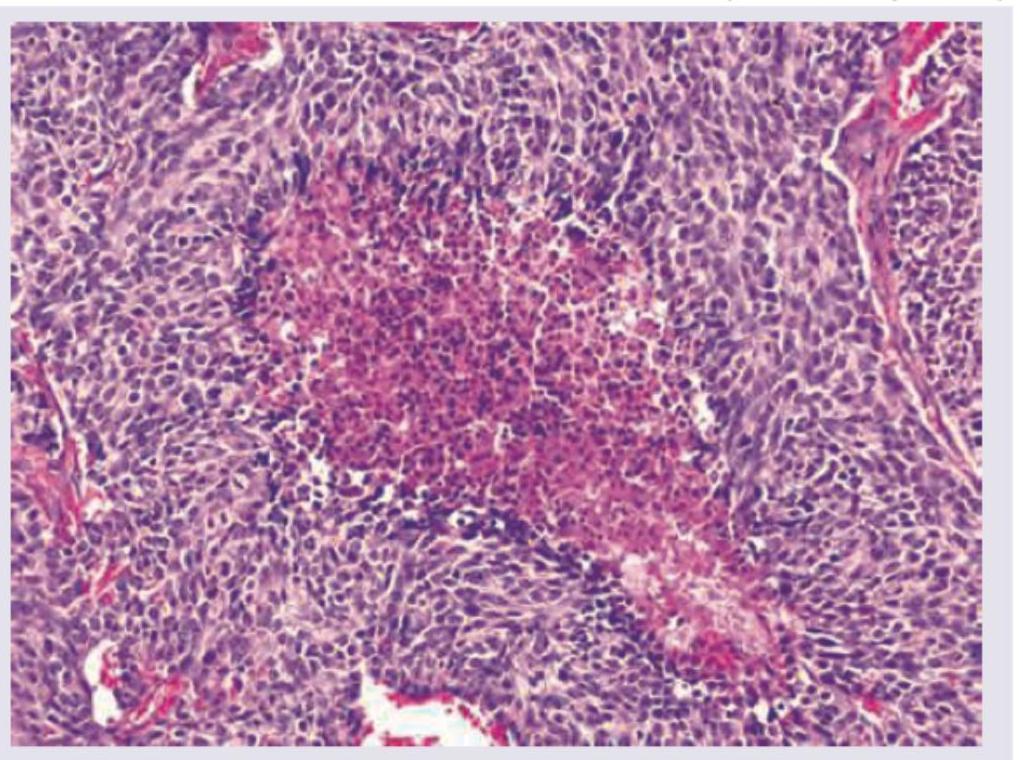
Question 2: A 55-year-old male patient presented with a 4 month history of cough and hemoptysis. Bronchoscopy revealed an intrabronchial polyp. Biopsy from the polyp showed small cells with salt and pepper chromatin, with microscopic necrosis and 5 mitotic figures per 10 high power fields as shown below. Chromogranin staining was positive. What is the diagnosis and grade of the lesion?
- A. Carcinoid grade 1
- B. Small cell carcinoma grade IV
- C. Large cell neuroendocrine carcinoma grade IV
- D. Atypical carcinoid grade 2 (Correct Answer)
Explanation: ***Atypical carcinoid grade 2*** - The presence of **salt and pepper chromatin**, **microscopic necrosis**, and **5 mitotic figures per 10 high power fields** are characteristic features of an **atypical carcinoid tumor** [1]. - **Positive chromogranin staining** confirms neuroendocrine differentiation, and the mitotic rate coupled with necrosis indicates a Grade 2 (atypical) carcinoid based on WHO classification [1]. *Carcinoid grade 1* - A typical carcinoid (Grade 1) would show **no necrosis** and a mitotic count of **less than 2 mitoses per 10 high power fields**, which contradicts the findings [1]. - While it features **salt and pepper chromatin** and positive neuroendocrine markers, the higher mitotic activity and necrosis exclude a typical carcinoid. *Small cell carcinoma grade IV* - **Small cell carcinoma** typically presents with extensive necrosis, very high mitotic activity (often >10 mitoses/10 HPF), and a more **scanty cytoplasm** than seen here, and often **crush artifact** [2]. - Although it is a high-grade neuroendocrine tumor, the described features (only 5 mitoses/10HPF, "salt and pepper chromatin" is less typical for SCLC which has more uniform nuclei, and distinct necrosis without widespread crush artifact) are more consistent with an atypical carcinoid [1], [2]. *Large cell neuroendocrine carcinoma grade IV* - **Large cell neuroendocrine carcinoma** (LCNEC) is characterized by **large cells** with prominent nucleoli, high mitotic counts (often >10-11 mitoses/10HPF), and extensive necrosis [2]. - The "small cells" and **salt and pepper chromatin** described in the biopsy are inconsistent with the large cell morphology of LCNEC. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 725-727. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 337-338.
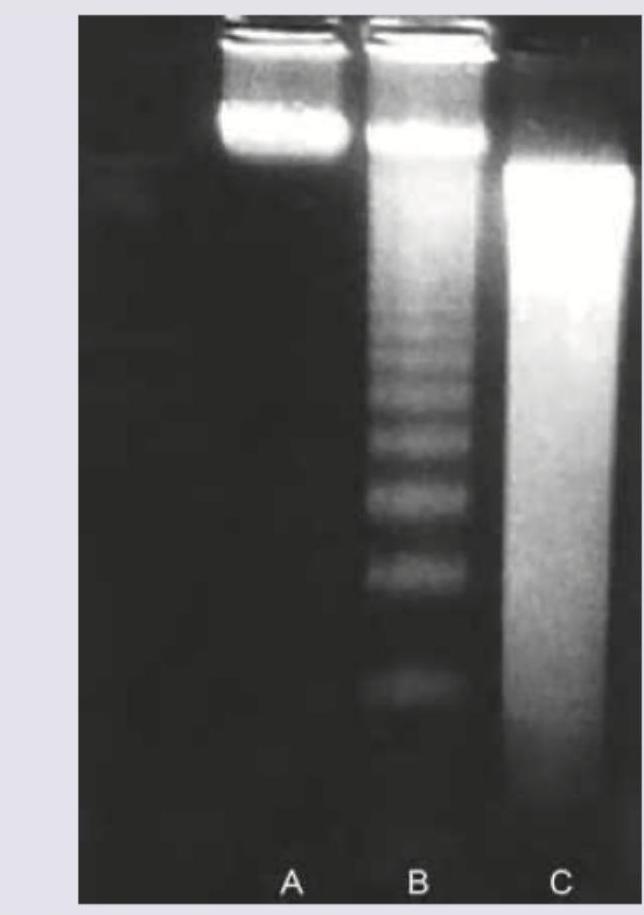
Question 3: Agarose gel electrophoresis from DNA of a population of cells as seen under ultraviolet light is shown below. What is the correct explanation for the finding seen in the band labeled as "C"?
- A. Predominantly necrotic cells
- B. Mixed population of normal and apoptotic cells
- C. A population of viable cells
- D. Apoptotic cells (Correct Answer)
Explanation: ***Apoptotic cells*** - Band C shows a characteristic **DNA ladder pattern** with discrete bands representing fragmentation into nucleosome-sized units (multiples of ~180-200 base pairs), which is pathognomonic of **apoptosis**. [1] - During apoptosis, **endonucleases** cleave DNA at internucleosomal linker regions, creating uniform fragments that migrate as distinct bands on agarose gel electrophoresis. *Predominantly necrotic cells* - **Necrotic cell DNA** undergoes random, non-specific degradation by cellular enzymes, resulting in a continuous **smear pattern** rather than discrete bands. - The **smear appearance** reflects DNA fragments of varying sizes distributed throughout the gel, unlike the organized pattern seen in band C. *Mixed population of normal and apoptotic cells* - A mixed population would show both **intact high molecular weight DNA** (remaining near the gel origin) and the **apoptotic ladder pattern** superimposed. - Band C displays a pure ladder pattern without evidence of intact DNA, indicating a homogeneous apoptotic population. *A population of viable cells* - **Viable cells** maintain intact genomic DNA that remains as a single **high molecular weight band** near the top of the gel. - The **fragmented ladder pattern** in band C is incompatible with viable cell DNA, which should show minimal degradation. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Cellular Responses to Stress and Toxic Insults: Adaptation, Injury, and Death, pp. 63-64.
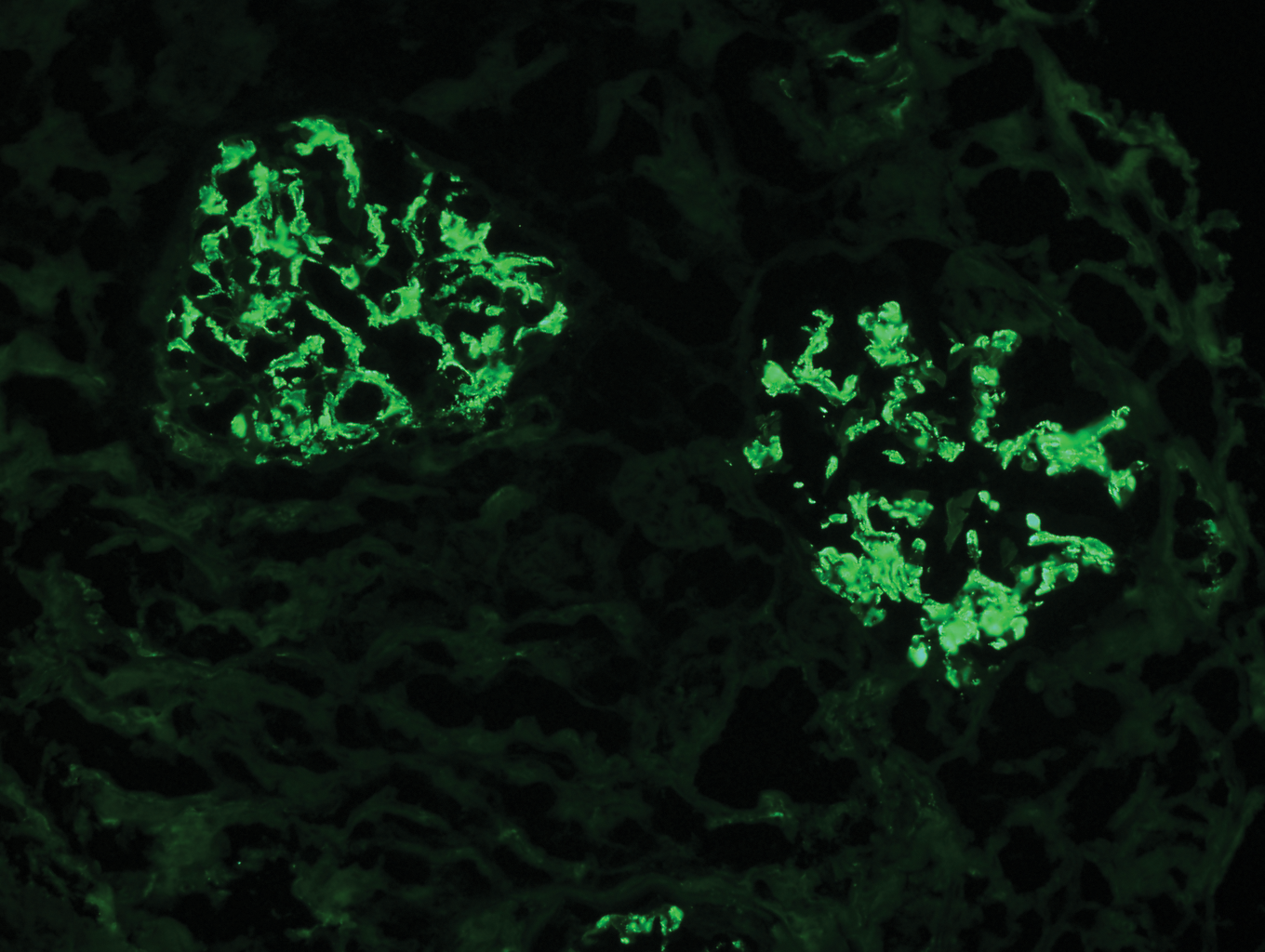
Question 4: The following is the FITC for IgG stained kidney specimen. What is this suggestive of?
- A. SLE (Correct Answer)
- B. Post-streptococcal glomerulonephritis
- C. Goodpasture syndrome
- D. Membranous glomerulonephritis
- E. IgA nephropathy
Explanation: ***SLE*** - **Lupus nephritis** (a kidney manifestation of SLE) often shows a "full house" immunofluorescence pattern, including **IgG deposition**, along with IgA, IgM, C3, and C1q [1]. - The presence of **IgG staining** in a kidney biopsy is a common finding in various forms of lupus nephritis, such as diffuse proliferative glomerulonephritis [1,5]. *Buerger's disease* - This is a **vasculitis** primarily affecting small and medium-sized arteries and veins, typically in the limbs. - It does **not primarily involve the kidneys** with IgG deposition and is not diagnosed via kidney biopsy immunofluorescence. *Goodpasture syndrome* - Characterized by **linear deposition of IgG** along the glomerular basement membrane (GBM) on immunofluorescence. - While it involves IgG, the question implies a more general IgG staining, and Goodpasture's has a very specific **linear pattern**, which is distinct from the granular or mesangial patterns often seen in SLE [2]. *Membranous glomerulonephritis* - This condition is characterized by **granular subepithelial deposits of IgG and C3** along the glomerular basement membrane [1]. - While it involves IgG, the question's image (if implied) would likely show a more diffuse, granular pattern, and SLE can also present with IgG, but often with other immune complex components, making SLE a broader and often more complex picture [2]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 532-533. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, p. 911. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of the Immune System, pp. 230-232.
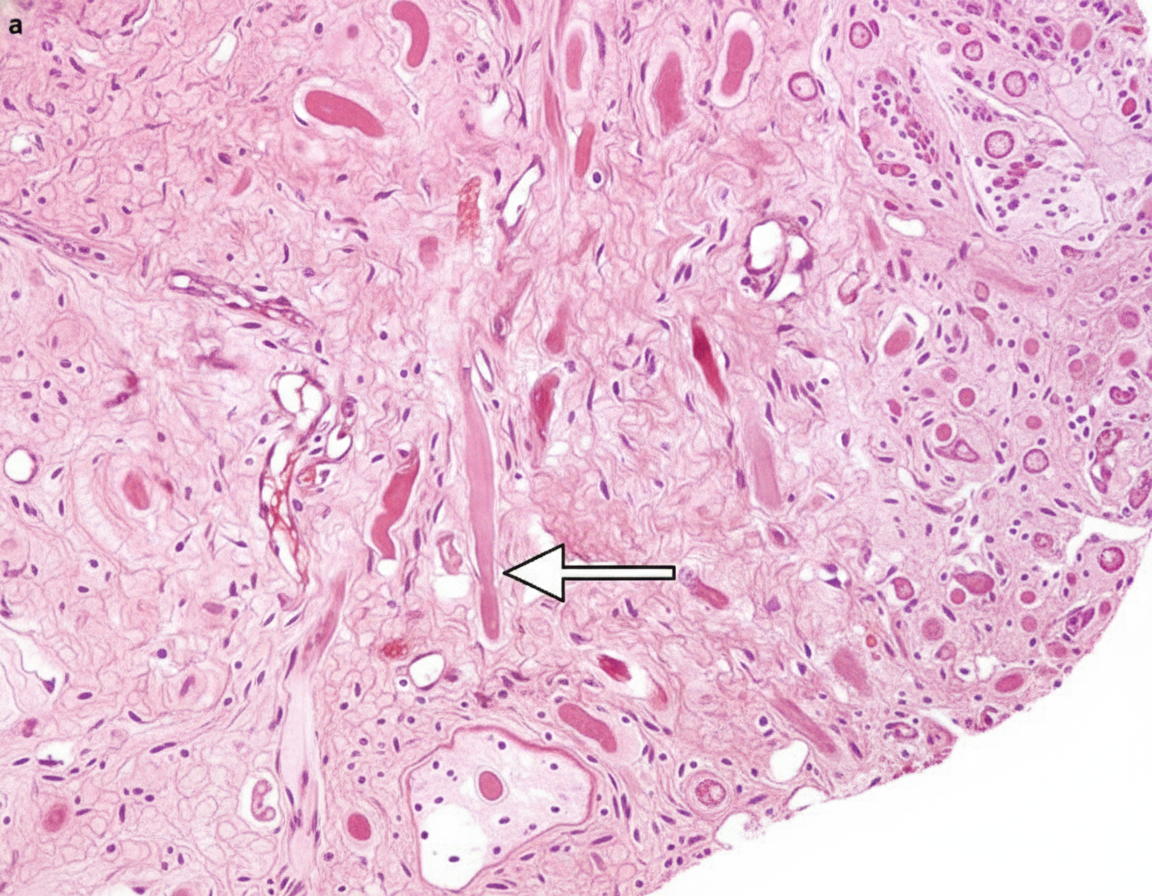
Question 5: The following microscopic appearance is that of a schwannoma which most commonly involves the cerebellopontine angle. What does the area marked with the arrow represent?
- A. Antony A pattern
- B. Antony B pattern (Correct Answer)
- C. Antony C pattern-Verocay cells
- D. Antony D pattern-Verocay cells
- E. Verocay bodies
Explanation: ***Antony B pattern-Verocay cells*** - The area marked with the arrow represents **Antony B pattern**, which is characterized by **hypocellularity** and a **myxoid matrix** [1]. - **Verocay bodies** are specific to schwannomas and are formed by palisading nuclei surrounding an anucleate zone, typically found within the **Antony A pattern** [1]. *Antony A pattern* - **Antony A pattern** is characterized by **dense cellularity** with palisading nuclei and often contains **Verocay bodies** [1]. - This pattern is typically more organized and compact compared to the area shown. *Antony C pattern-Verocay cells* - There is no recognized **Antony C pattern** in the histological classification of schwannomas. - The primary patterns described are **Antony A** and **Antony B**. *Antony D pattern-Verocay cells* - Similar to Antony C, there is no recognized **Antony D pattern** in the histological classification of schwannomas. - This option is a distractor based on an incorrect classification. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, p. 1250.
Pharmacology
1 questionsMethacholine acts primarily at which receptor?
INI-CET 2015 - Pharmacology INI-CET Practice Questions and MCQs
Question 1: Methacholine acts primarily at which receptor?
- A. M1
- B. M2
- C. M3 (Correct Answer)
- D. M4
Explanation: ***M3*** - **Methacholine** is a non-selective muscarinic agonist that acts at all muscarinic receptors, but its **primary clinically relevant effects**, particularly in the airways (e.g., bronchoconstriction in asthma challenge tests), are mediated through **M3 receptors**. - **M3 receptors** are Gq-coupled and lead to **smooth muscle contraction**, glandular secretion, and vasodilation via nitric oxide release. *M1* - **M1 receptors** are primarily found in the central nervous system and autonomic ganglia, playing a role in **neuronal excitation** and **autonomic transmission**. - While methacholine can activate M1 receptors, this is not its predominant site of action for clinical uses. *M2* - **M2 receptors** are found in the heart and are Gi-coupled, leading to a **decrease in heart rate** and contractility. - While methacholine acts on M2 receptors, its most notable effects (like bronchoconstriction) are not primarily mediated through M2. *M4* - **M4 receptors** are primarily located in the central nervous system, where they modulate neurotransmitter release and contribute to **motor control** and cognition. - Methacholine has some affinity for M4, but it is not the primary receptor responsible for its clinically relevant effects.
Radiology
3 questionsIdentify the ECG given in the figure below.
A patient presents with neck pain and rigidity which gets relieved after bathing in hot water and exercise. Cervical X-ray is shown below. What is your diagnosis?

In the condition shown below, rib notching is present in which of the following ribs? (AIIMS Nov 2015)
INI-CET 2015 - Radiology INI-CET Practice Questions and MCQs
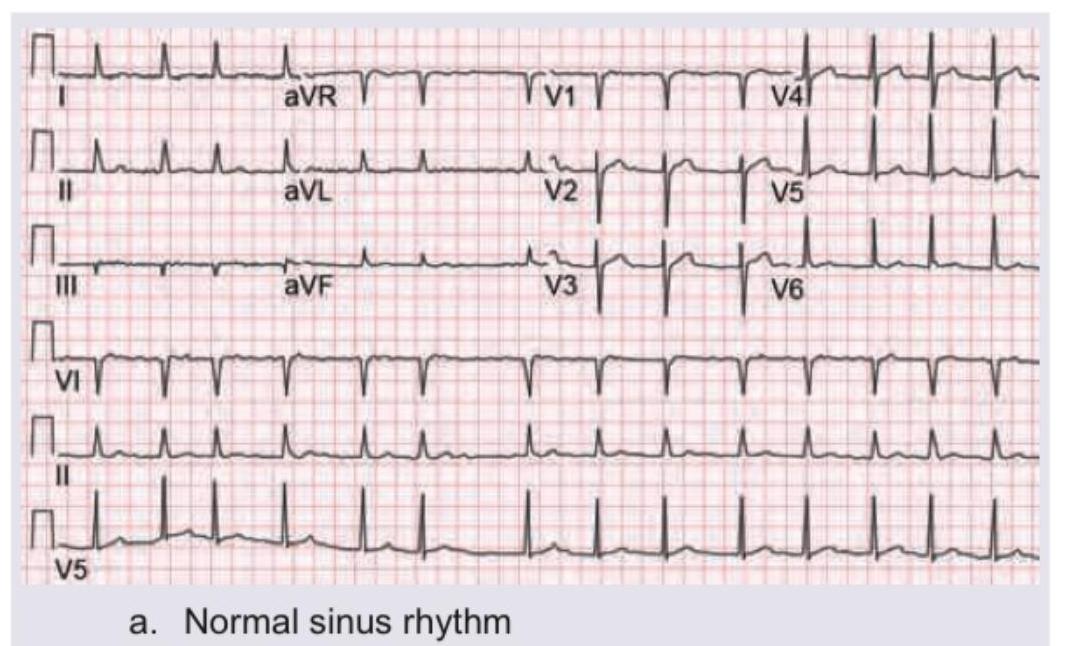
Question 1: Identify the ECG given in the figure below.
- A. Normal sinus rhythm (Correct Answer)
- B. Paroxysmal supraventricular tachycardia
- C. Atrial fibrillation
- D. Ventricular fibrillation
Explanation: ***Normal sinus rhythm*** - The ECG shows regular **P waves** followed by **QRS complexes**, with a consistent PR interval and a heart rate between 60-100 beats per minute, which are all characteristics of a normal sinus rhythm. - The QRS complexes are narrow, indicating normal ventricular depolarization, and the T waves are appropriately configured. *Paroxysmal supraventricular tachycardia* - This rhythm would typically show a **very rapid heart rate** (150-250 bpm) with narrow QRS complexes and often obscured or absent P waves. - The rate in this ECG is clearly within the normal range, and P waves are distinctly visible before each QRS. *Atrial fibrillation* - Atrial fibrillation is characterized by an **irregularly irregular rhythm**, absence of distinct P waves, and an erratic baseline due to chaotic atrial activity. - This ECG clearly shows a regular rhythm with discernible P waves. *Ventricular fibrillation* - Ventricular fibrillation is a life-threatening arrhythmia characterized by completely **chaotic and irregular electrical activity** in the ventricles, resulting in no identifiable P waves, QRS complexes, or T waves. - The ECG in the image shows clearly defined, organized waveforms, making ventricular fibrillation incorrect.
Question 2: A patient presents with neck pain and rigidity which gets relieved after bathing in hot water and exercise. Cervical X-ray is shown below. What is your diagnosis?
- A. Spondylolisthesis
- B. Spondylosis
- C. Spondylitis (Correct Answer)
- D. Spondyloptosis
Explanation: ***Spondylitis (Ankylosing Spondylitis)*** - The image shows **fusion of vertebral bodies** (ankylosis) and an appearance consistent with a **bamboo spine**, which is characteristic of advanced **Ankylosing Spondylitis**. - The clinical presentation is pathognomonic: **inflammatory back pain with morning stiffness** that is **relieved by activity and hot water bathing** (as opposed to mechanical pain which worsens with activity). - This is a classic presentation of inflammatory spondyloarthropathy, specifically ankylosing spondylitis. *Spondylolisthesis* - This condition involves the **slippage of one vertebra over another**, which is not the primary finding on this X-ray. - While spondylolisthesis can cause neck pain, it does **not typically present with diffuse vertebral fusion** as seen here, and the pain would worsen with activity (mechanical pattern), not improve. *Spondylosis* - Spondylosis refers to **degenerative changes** of the spine, often involving **osteophytes** and **disc space narrowing**. - While some degenerative changes may be present, the pronounced fusion and **"bamboo spine" appearance** go beyond typical spondylosis and indicate an inflammatory process. - Degenerative pain typically **worsens with activity**, unlike the relief with exercise seen in this patient. *Spondyloptosis* - Spondyloptosis is an **extreme form of spondylolisthesis** where one vertebra has completely slipped off the one below it (Grade V slip). - This severe displacement is not apparent on the X-ray; instead, there is **fusion rather than translational instability**.
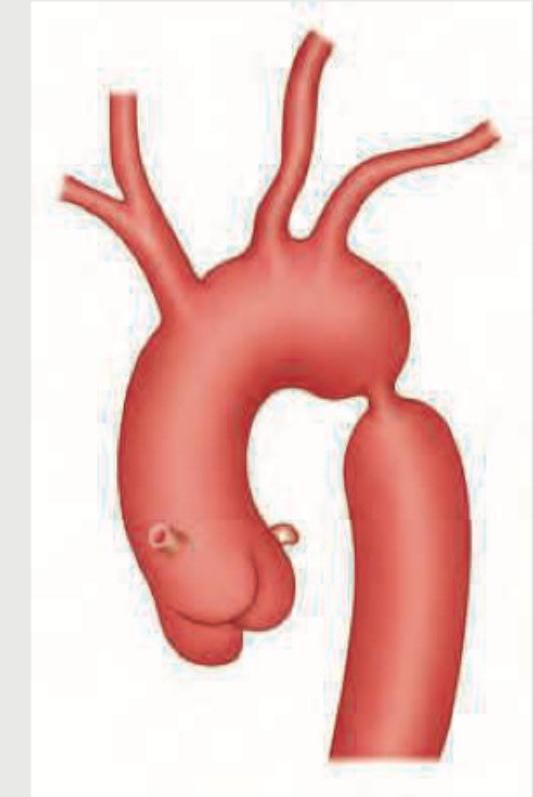
Question 3: In the condition shown below, rib notching is present in which of the following ribs? (AIIMS Nov 2015)
- A. 3rd to 9th ribs (Correct Answer)
- B. 1st to 9th ribs
- C. 11th and 12th ribs
- D. All ribs
Explanation: **3rd to 9th ribs** - The image provided depicts **coarctation of the aorta**, characterized by a narrowing of the aorta, typically distal to the origin of the left subclavian artery. - In coarctation of the aorta, collateral circulation develops through the **intercostal arteries** to bypass the constriction, leading to their enlargement and subsequent erosion of the inferior margins of the **3rd to 9th ribs**, a finding known as "rib notching." *1st to 9th ribs* - While rib notching affects upper ribs, it typically **spares the 1st and 2nd ribs** because the superior intercostal arteries (which supply these ribs) originate directly from the subclavian artery, often proximal to the coarctation, so they do not participate in collateral circulation as significantly. - The pattern of notching is usually more concentrated in the mid-thoracic region. *11th and 12th ribs* - Rib notching from coarctation of the aorta is rarely observed in the **floating ribs** (11th and 12th ribs). - These ribs have a different anatomical relationship with the pleura and typically do not bear the brunt of increased collateral flow from the intercostal arteries in the same way as the higher ribs. *All ribs* - Rib notching is a localized phenomenon reflecting increased blood flow through specific intercostal arteries involved in collateral circulation due to aortic coarctation. - Therefore, it does **not affect all ribs**, and its absence in certain ribs (like the 1st, 2nd, 11th, and 12th) helps differentiate this condition radiologically.
About INI-CET 2015 Questions
This page contains 36 questions from the INI-CET 2015 paper, organised across 15 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the INI-CET exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your INI-CET goals.