INI-CET 2014
13 Previous Year Questions with Answers & Explanations
Biochemistry
1 questionsWhich of the following induces apoptosis in a cell?
INI-CET 2014 - Biochemistry INI-CET Practice Questions and MCQs
Question 1: Which of the following induces apoptosis in a cell?
- A. Glucocorticoids (Correct Answer)
- B. Isoprenoids
- C. Myristic acid
- D. Oleic acid
Explanation: ***Glucocorticoids*** - **Glucocorticoids** are known to induce apoptosis in various cell types, particularly lymphocytes, making them useful in **lymphoid malignancies**. - They activate a complex signaling pathway that leads to the activation of pro-apoptotic proteins and the suppression of anti-apoptotic proteins, ultimately resulting in **programmed cell death**. *Isoprenoids* - **Isoprenoids** are a large class of organic compounds derived from isoprene, involved in various metabolic processes like cholesterol synthesis and protein prenylation, but do not directly induce apoptosis. - While some isoprenoid precursors or inhibitors of isoprenoid synthesis can affect cell proliferation or survival, isoprenoids themselves are not primary apoptosis inducers. *Myristic acid* - **Myristic acid** is a saturated fatty acid primarily involved in protein myristoylation, a post-translational modification essential for various cellular functions. - It is not known to be a direct inducer of apoptosis but can influence signaling pathways that may indirectly impact cell survival or death. *Oleic acid* - **Oleic acid** is a monounsaturated fatty acid that is a major component of cell membranes and is involved in energy storage and signaling. - It is generally considered cytoprotective and can even inhibit apoptosis in some contexts, rather than inducing it.
Forensic Medicine
1 questionsIn an act of tribadism, the active partner is known as: (AIIMS 12; COMEDK 14)
INI-CET 2014 - Forensic Medicine INI-CET Practice Questions and MCQs
Question 1: In an act of tribadism, the active partner is known as: (AIIMS 12; COMEDK 14)
- A. Butch (Correct Answer)
- B. Bugger
- C. Femme
- D. Catamite
Explanation: ***Butch*** - While this answer reflects the terminology used in the original examination, it's important to note that **"butch"** is primarily a **sociocultural identity term** describing masculine gender expression in lesbian relationships, rather than standard forensic medicine terminology. - In classical forensic medicine literature, the active partner in tribadism is more accurately termed a **"tribade"** (from Greek "tribein" = to rub). - Tribadism refers to a form of **female same-sex sexual activity** where the active partner achieves sexual gratification by **rubbing or pressing the vulva** against another woman's body, particularly the thigh, pubic region, or vulva. - This question reflects **historical exam terminology** rather than current forensic medicine standards. *Bugger* - This is an archaic/derogatory term historically used for a person who performs **anal intercourse** (buggery/sodomy). - The term is associated with **male same-sex activity** or unnatural sexual offenses under older legal frameworks. - It is **not related to tribadism**, which involves female same-sex activity without penetration. *Femme* - This is a sociocultural term describing the more **feminine-presenting partner** in some lesbian relationships. - It refers to **gender expression/identity**, not a forensic medicine classification of sexual acts. - This is **not standard medicolegal terminology** for describing roles in tribadism. *Catamite* - A catamite refers to a **young boy kept for homosexual purposes**, historically associated with pederasty in ancient civilizations. - This term is related to **male same-sex activity** and is entirely **irrelevant to tribadism**, which is a form of female same-sex sexual activity. - This is an archaic term rarely used in modern forensic medicine.
General Medicine
1 questionsA 65-year-old elderly male has history of sweating and chest pain for last 24 hr with the following ECG. Which of the following is not given in managing the patient?
INI-CET 2014 - General Medicine INI-CET Practice Questions and MCQs
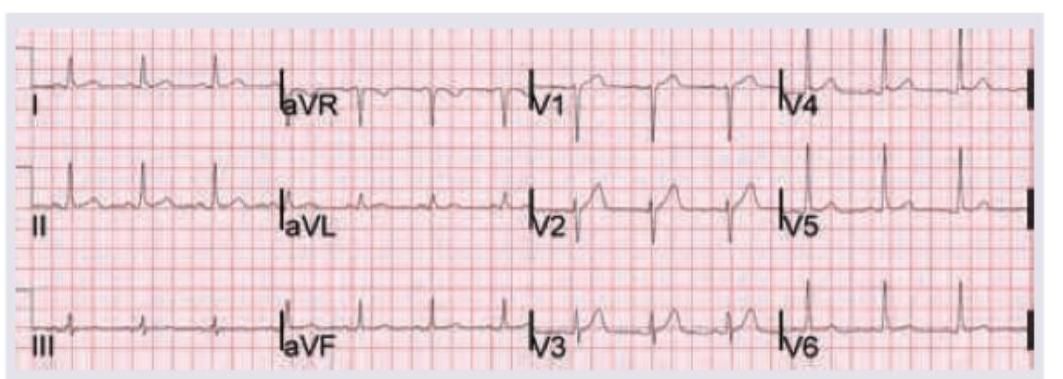
Question 1: A 65-year-old elderly male has history of sweating and chest pain for last 24 hr with the following ECG. Which of the following is not given in managing the patient?
- A. Aspirin
- B. Statin
- C. Thrombolytic therapy (Correct Answer)
- D. Morphine
Explanation: ***Thrombolytic therapy*** - **Thrombolytic therapy** is contraindicated in this patient due to the **24-hour delay** from symptom onset, as fibrinolytic therapy is generally not recommended beyond **12 hours** and absolutely contraindicated after **24 hours**. - The **risk-benefit ratio** becomes unfavorable after this time window, with increased bleeding risk and minimal myocardial salvage potential, making **primary PCI** the preferred reperfusion strategy if available. *Aspirin* - **Aspirin** remains indicated in STEMI regardless of presentation timing as an **antiplatelet agent**. - It provides ongoing **secondary prevention** benefits and helps prevent further thrombotic events even in delayed presentations. *Statin* - **High-dose statin therapy** is recommended immediately in all ACS patients, including those with delayed presentation. - Statins provide **plaque stabilization** and **anti-inflammatory effects** that are beneficial regardless of symptom onset timing. *Morphine* - While **morphine** is generally avoided in STEMI due to potential **delayed absorption** of oral antiplatelet agents and possible increased mortality, it may still be considered for **severe refractory chest pain**. - It can be used cautiously when **nitroglycerin** fails to provide adequate pain relief, especially in delayed presentations where reperfusion options are limited.
Internal Medicine
2 questionsCommonest cause of thunderclap headache:
A 65-year-old elderly male with the ECG shown below has a history of sweating and chest pain for the last 24 hrs . Which of the following is not given in managing the patient?
INI-CET 2014 - Internal Medicine INI-CET Practice Questions and MCQs
Question 1: Commonest cause of thunderclap headache:
- A. Basilar migraine
- B. Extradural hemorrhage
- C. Subdural hemorrhage
- D. Aneursymal SAH (Correct Answer)
Explanation: ***Aneursymal SAH*** - An **aneurysmal subarachnoid hemorrhage (SAH)** is the most common and often life-threatening cause of a **thunderclap headache**, characterized by a sudden, severe headache reaching maximum intensity within one minute [1]. - The sudden rupture of a cerebral aneurysm leads to blood spilling into the subarachnoid space, causing a rapid increase in intracranial pressure and meningeal irritation. *Basilar migraine* - While basilar migraine can cause severe headaches, it typically presents with neurological symptoms like **vertigo**, **ataxia**, and **diplopia** preceding the headache phase, and its onset is usually less abrupt than a thunderclap headache. - Basilar migraines usually have a **recurrent pattern** and are associated with a history of similar migraine episodes, unlike the abrupt, singular nature of an SAH-related thunderclap headache. *Extradural hemorrhage* - An **extradural (epidural) hemorrhage** is usually caused by **head trauma** and often presents with a **lucid interval** followed by a progressive neurological decline, rather than an immediate thunderclap headache [2]. - It involves bleeding between the **dura mater** and the skull, which typically develops more slowly than the catastrophic onset of an SAH. *Subdural hemorrhage* - A **subdural hemorrhage** is usually caused by **venous bleeding** and can be acute, subacute, or chronic, often presenting with a gradual onset of symptoms like headache, confusion, and neurological deficits [2]. - While an acute subdural hematoma can be severe, its headache is generally not as instantaneously explosive or universally described as a thunderclap as that seen with SAH.
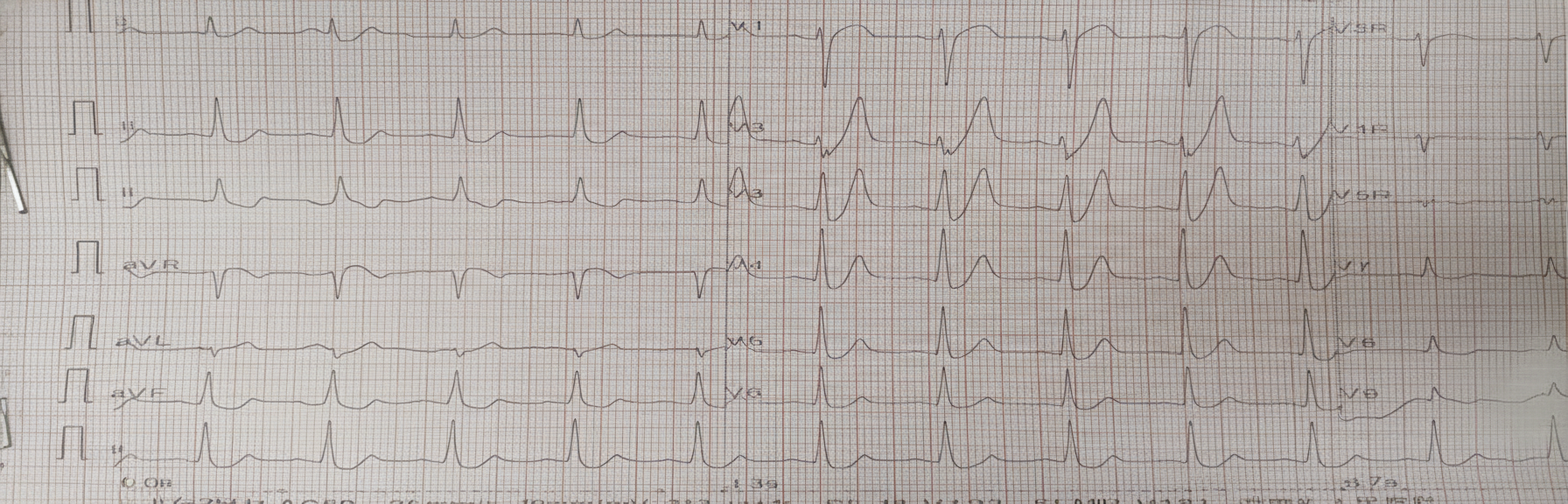
Question 2: A 65-year-old elderly male with the ECG shown below has a history of sweating and chest pain for the last 24 hrs . Which of the following is not given in managing the patient?
- A. Aspirin
- B. Statin
- C. Thrombolytic therapy (Correct Answer)
- D. Morphine
- E. Beta-blockers
Explanation: ***Thrombolytic therapy*** - The ECG shows significant **Q waves** and **T-wave inversion** in inferolateral leads (II, III, aVF, V5, V6), indicating an **evolving or established myocardial infarction** (MI), not an acute ST-elevation MI (STEMI suitable for immediate thrombolysis). - Given the symptoms began 24 hours ago, the patient is likely outside the optimal window for thrombolytic therapy, which is most effective within **12 hours** of symptom onset for STEMI. After 12-24 hours, the benefits are marginal, and risks of bleeding increase. *Aspirin* - **Aspirin** is an integral part of NSTEMI/STEMI management as an **antiplatelet agent**, given to almost all patients who are not allergic, regardless of time of presentation. - It works by **inhibiting cyclooxygenase** and thereby reducing platelet aggregation, preventing further clot formation. *Statin* - **Statins** are initiated early in MI management, even in the acute phase, for their **pleiotropic effects** beyond lipid-lowering, including **stabilizing plaques** and reducing inflammation. - Long-term statin therapy is crucial for **secondary prevention** in patients with established coronary artery disease. *Morphine* - **Morphine** is often used in the acute management of MI for **pain relief** and can also provide some **venodilation**, reducing preload and myocardial oxygen demand. - While typically used during the active chest pain phase, it remains an option for symptom management if pain persists, even after 24 hours. *Beta-blockers* - **Beta-blockers** are a cornerstone of post-MI management, started within the first 24 hours in hemodynamically stable patients without contraindications. - They reduce **myocardial oxygen demand**, prevent arrhythmias, and improve long-term survival. - Standard therapy even at 24 hours post-MI presentation.
Ophthalmology
1 questionsWhich cells are affected in glaucomatous optic neuropathy?
INI-CET 2014 - Ophthalmology INI-CET Practice Questions and MCQs
Question 1: Which cells are affected in glaucomatous optic neuropathy?
- A. Amacrine cells
- B. Bipolar cells
- C. Ganglion cells (Correct Answer)
- D. Rods and cones
Explanation: **Explanation:** **Glaucomatous Optic Neuropathy (GON)** is characterized by progressive damage to the optic nerve, primarily involving the **Retinal Ganglion Cells (RGCs)** and their axons. 1. **Why Ganglion Cells are correct:** The pathophysiology of glaucoma involves mechanical compression (due to elevated Intraocular Pressure) and vascular ischemia at the lamina cribrosa. This leads to the **apoptosis (programmed cell death)** of Retinal Ganglion Cells. Since the axons of these RGCs converge to form the optic nerve, their loss results in the characteristic "cupping" of the optic disc and corresponding visual field defects. 2. **Why other options are incorrect:** * **Amacrine and Bipolar cells:** These are interneurons located in the inner nuclear layer of the retina. While some secondary degeneration may occur in advanced stages, they are not the primary site of injury in glaucoma. * **Rods and Cones:** These are photoreceptors located in the outermost layer of the retina. They are responsible for converting light into electrical signals. Glaucoma is a disease of the "inner retina" (output neurons), whereas diseases like Retinitis Pigmentosa primarily affect the photoreceptors. **Clinical Pearls for NEET-PG:** * **Earliest Change:** The earliest structural change in glaucoma is often the thinning of the **Retinal Nerve Fiber Layer (RNFL)**, which consists of RGC axons. * **Mechanism of Death:** RGC death in glaucoma occurs via **Apoptosis**, triggered by neurotrophin deprivation and glutamate excitotoxicity. * **Diagnostic Tool:** **Optical Coherence Tomography (OCT)** is used to quantify the loss of the Ganglion Cell Complex (GCC) and RNFL thickness for early diagnosis.
Pediatrics
2 questionsA 7-year-old girl is easily distracted in class and exhibits poor scholastic performance. EEG shows? (AIIMS May 2014)
A 6-week-old baby presents with cough and cold for the past 3 days. The respiratory rate is 48/min. On examination, the patient is febrile with wheezing but no chest indrawing. Which of the following statements is not true?
INI-CET 2014 - Pediatrics INI-CET Practice Questions and MCQs
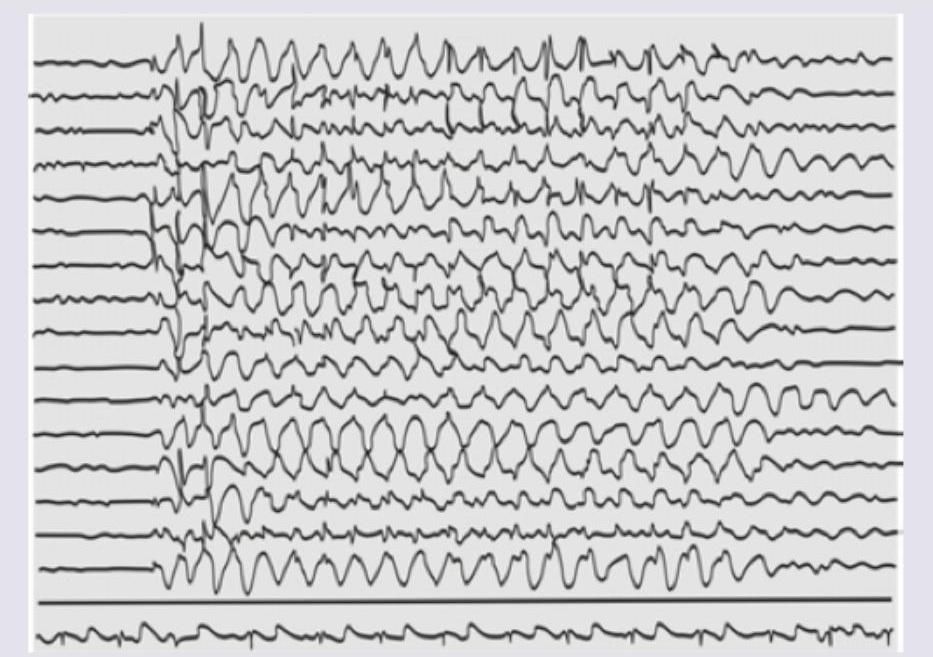
Question 1: A 7-year-old girl is easily distracted in class and exhibits poor scholastic performance. EEG shows? (AIIMS May 2014)
- A. Myoclonic seizures
- B. Absence seizures (Correct Answer)
- C. Atonic seizures
- D. Myoclonia
Explanation: ***Absence seizures*** - The clinical presentation of a young girl who is **easily distracted** and has **poor scholastic performance** is highly suggestive of absence seizures. These are brief episodes of impaired consciousness often mistaken for daydreaming. - The EEG image shows a characteristic **generalized 3-Hz spike-and-wave discharge** pattern, which is the hallmark of typical absence seizures. *Myoclonic seizures* - Myoclonic seizures involve **sudden, brief muscle jerks** or twitches, which are not described in the patient's presentation. - The EEG in myoclonic seizures typically shows **polyspike-and-wave discharges**, not the 3-Hz spike-and-wave pattern seen here. *Atonic seizures* - Atonic seizures, also known as **drop attacks**, cause a sudden loss of muscle tone leading to falls, which is not consistent with the described symptoms. - While EEG may show generalized spike-and-wave activity or diffuse slow waves during an atonic seizure, the 3-Hz rhythmic pattern is less typical for this seizure type. *Myoclonia* - Myoclonia refers to **involuntary, sudden muscle contractions**, which can be physiological (e.g., hiccups, sleep starts) or pathological. - While myoclonic seizures are a type of myoclonia, the term "myoclonia" alone is too general and does not specifically align with the classic EEG pattern and subtle clinical signs of absence seizures.
Question 2: A 6-week-old baby presents with cough and cold for the past 3 days. The respiratory rate is 48/min. On examination, the patient is febrile with wheezing but no chest indrawing. Which of the following statements is not true?
- A. The child has pneumonia. (Correct Answer)
- B. Antibiotics are not required.
- C. Wheezing should be treated.
- D. Fever should be treated.
Explanation: ### Explanation The core of this question lies in the **WHO Integrated Management of Neonatal and Childhood Illness (IMNCI)** guidelines for classifying respiratory infections. **1. Why "The child has pneumonia" is NOT true:** According to WHO/IMNCI criteria for a child aged 2 months to 5 years, pneumonia is defined by **fast breathing** or **chest indrawing**. For a child aged **2 months to 12 months**, the cutoff for fast breathing is **≥ 50 breaths/min**. In this case, the 6-week-old (1.5 months) infant has a respiratory rate of **48/min**, which is **normal** (the cutoff for infants < 2 months is ≥ 60/min). Since there is no fast breathing and no chest indrawing, the child is classified as having a **"No Pneumonia" (Cough or Cold)**. **2. Analysis of other options:** * **Antibiotics are not required:** True. Since the diagnosis is a simple cough/cold (likely viral bronchiolitis or URTI), antibiotics are not indicated. * **Wheezing should be treated:** True. Wheezing in an infant indicates airway obstruction (often Bronchiolitis). Supportive care or a trial of bronchodilators is appropriate. * **Fever should be treated:** True. Symptomatic management of fever (e.g., Paracetamol) is standard care to ensure the infant's comfort and hydration. **Clinical Pearls for NEET-PG:** * **IMNCI Respiratory Rate Cutoffs:** * < 2 months: ≥ 60/min (Fast breathing) * 2–12 months: ≥ 50/min * 12 months–5 years: ≥ 40/min * **Classification Tip:** If a child has wheeze but no fast breathing/chest indrawing, it is managed as "No Pneumonia." If wheeze is present with fast breathing, treat with a bronchodilator first; if fast breathing persists after 3 doses, then classify as pneumonia.
Pharmacology
2 questionsMethacholine acts primarily at which receptor?
Which of the following conditions is NOT treated with a cholinomimetic agent?
INI-CET 2014 - Pharmacology INI-CET Practice Questions and MCQs
Question 1: Methacholine acts primarily at which receptor?
- A. M1
- B. M2
- C. M3 (Correct Answer)
- D. M4
Explanation: ***M3*** - **Methacholine** is a non-selective muscarinic agonist that acts at all muscarinic receptors, but its **primary clinically relevant effects**, particularly in the airways (e.g., bronchoconstriction in asthma challenge tests), are mediated through **M3 receptors**. - **M3 receptors** are Gq-coupled and lead to **smooth muscle contraction**, glandular secretion, and vasodilation via nitric oxide release. *M1* - **M1 receptors** are primarily found in the central nervous system and autonomic ganglia, playing a role in **neuronal excitation** and **autonomic transmission**. - While methacholine can activate M1 receptors, this is not its predominant site of action for clinical uses. *M2* - **M2 receptors** are found in the heart and are Gi-coupled, leading to a **decrease in heart rate** and contractility. - While methacholine acts on M2 receptors, its most notable effects (like bronchoconstriction) are not primarily mediated through M2. *M4* - **M4 receptors** are primarily located in the central nervous system, where they modulate neurotransmitter release and contribute to **motor control** and cognition. - Methacholine has some affinity for M4, but it is not the primary receptor responsible for its clinically relevant effects.
Question 2: Which of the following conditions is NOT treated with a cholinomimetic agent?
- A. Bradycardia (Correct Answer)
- B. Glaucoma
- C. Myasthenia gravis
- D. Post-surgical atony or ileus
Explanation: **Explanation:** Cholinomimetic agents (cholinergic agonists) mimic the action of acetylcholine (ACh) by stimulating muscarinic and nicotinic receptors. To answer this question, one must understand the physiological effects of Parasympathetic Nervous System (PNS) activation. **1. Why Bradycardia is the Correct Answer:** Stimulation of **M2 receptors** in the heart (specifically at the SA node) leads to a decrease in heart rate (negative chronotropy). Therefore, cholinomimetics would **worsen** bradycardia. In clinical practice, **anticholinergics** (like Atropine) are used to treat bradycardia, not cholinomimetics. **2. Why the other options are incorrect (Uses of Cholinomimetics):** * **Glaucoma:** Direct agonists like **Pilocarpine** cause miosis and contraction of the ciliary muscle, which opens the trabecular meshwork and facilitates the drainage of aqueous humor, reducing intraocular pressure. * **Myasthenia Gravis:** This condition involves autoantibodies against NMJ nicotinic receptors. Indirect cholinomimetics (AChE inhibitors) like **Pyridostigmine** or **Neostigmine** increase the concentration of ACh at the synaptic cleft, improving muscle strength. * **Post-surgical Atony/Ileus:** Drugs like **Bethanechol** (a muscarinic agonist) stimulate **M3 receptors** in the GI tract and bladder, promoting peristalsis and bladder emptying in non-obstructive conditions. **High-Yield NEET-PG Pearls:** * **Bethanechol:** "B" for Bowel and Bladder (used for postoperative ileus/urinary retention). * **Pilocarpine:** Drug of choice for acute angle-closure glaucoma. * **Edrophonium:** A short-acting AChE inhibitor used in the **Tensilon Test** for diagnosing Myasthenia Gravis (though largely replaced by antibody testing). * **Contraindications:** Cholinomimetics should be avoided in patients with **Asthma** (causes bronchoconstriction) and **Peptic Ulcer Disease** (increases gastric acid secretion).
About INI-CET 2014 Questions
This page contains 13 questions from the INI-CET 2014 paper, organised across 11 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the INI-CET exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your INI-CET goals.