All (607)Anatomy (42)Anesthesiology (16)Biochemistry (24)Community Medicine (55)Dermatology (14)ENT (18)Forensic Medicine (17)General Medicine (2)Internal Medicine (81)Microbiology (32)Obstetrics and Gynecology (59)Ophthalmology (25)Orthopaedics (11)Pathology (44)Pediatrics (40)Pharmacology (29)Physiology (18)Psychiatry (14)Radiology (21)Surgery (45)
Q71
OCPs are not protective for?
Q72
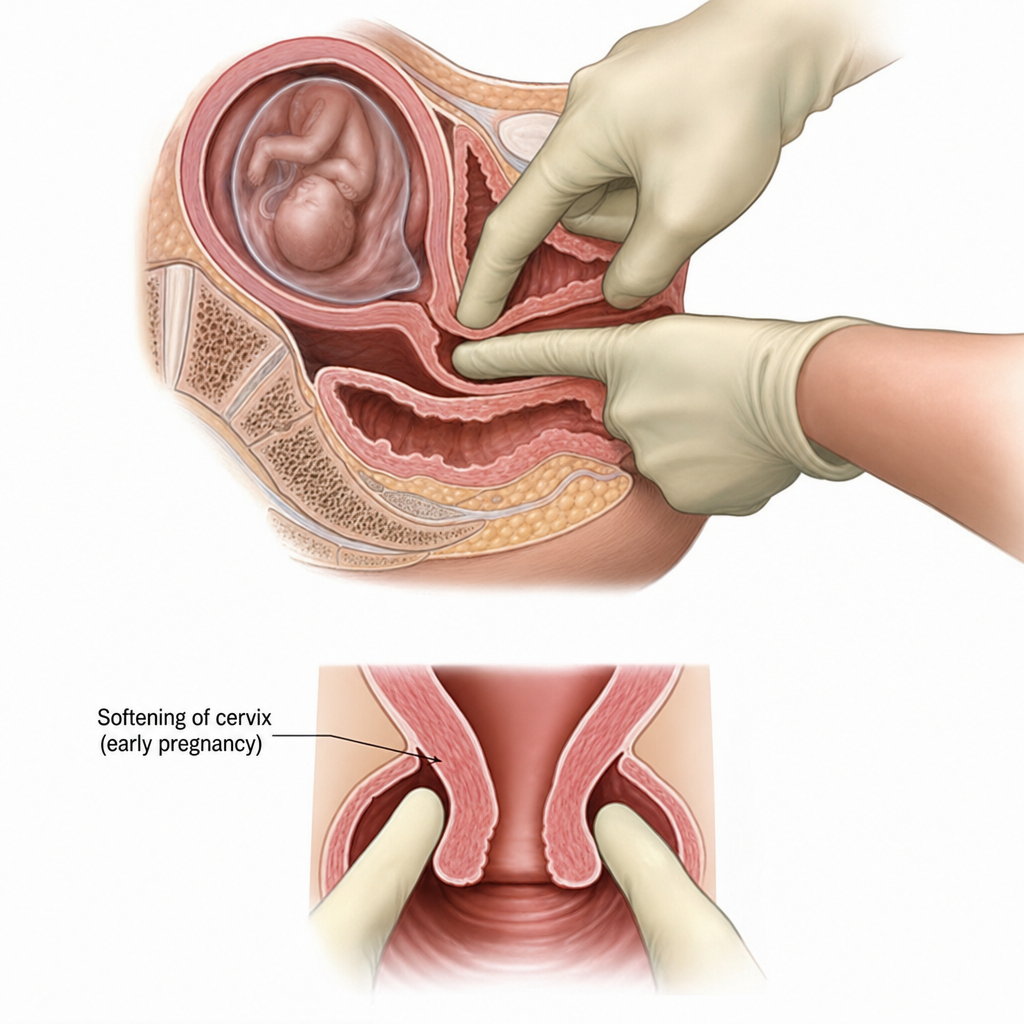
Which sign of pregnancy is demonstrated in the image below?
Q73
This instrument is contraindicated for?
Q74
The image depicts which of the following early signs of pregnancy?
Q75
Which findings are most suggestive of tubal pregnancy?
Q76
A female presents with hirsutism, delayed periods, obesity. USG findings are given below. What is the likely diagnosis?