All (606)Anatomy (42)Anesthesiology (16)Biochemistry (24)Community Medicine (55)Dermatology (14)ENT (18)Forensic Medicine (17)General Medicine (2)Internal Medicine (81)Microbiology (32)Obstetrics and Gynecology (59)Ophthalmology (25)Orthopaedics (11)Pathology (44)Pediatrics (40)Pharmacology (29)Physiology (18)Psychiatry (14)Radiology (21)Surgery (44)
Q461
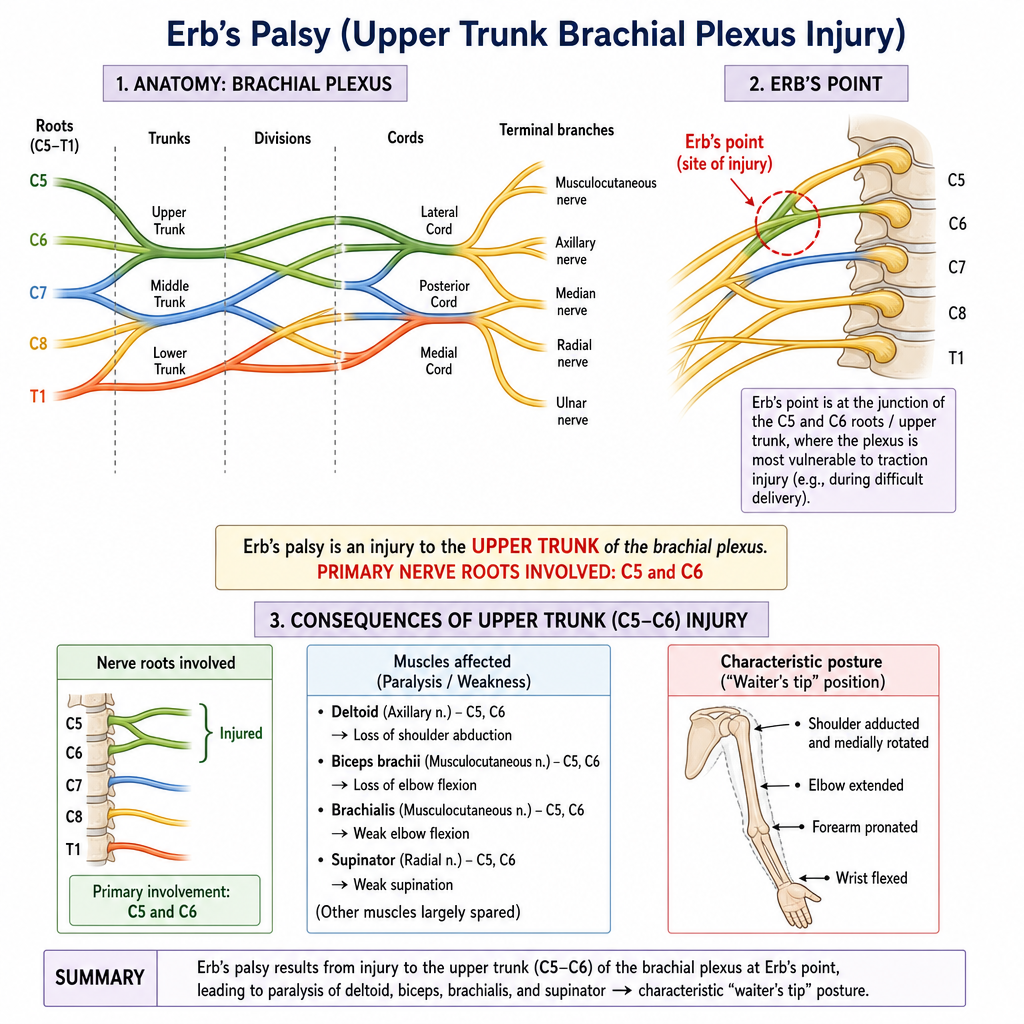
Identify the nerve roots involved in the condition depicted in the image.
Q462
A diabetic worker sustains a stab injury to the central region of his palm. After 3 days, he develops swelling, severe pain, and inability to extend his middle and ring fingers. Pus accumulation is suspected in one of the palmar spaces. Which of the following spaces is most likely involved?
Q463
Which is the narrowest part of the adult laryngeal airway?
Q464
A man sustained trauma on the lateral side of his right knee. Two days later, he complains of difficulty in walking, as his toes keep dragging on the ground. He also notices numbness over the upper lateral aspect of the leg and dorsum of the foot. Which nerve is most likely injured?
Q465
Refer to the images. A patient presents with the condition shown in . Which of the following nerve roots are primarily involved in this type of brachial plexus injury, often termed Erb's palsy, as indicated by Erb's point in the anatomical diagram ?
Q466
The upper part of the uncinate process commonly attaches to?