All (606)Anatomy (42)Anesthesiology (16)Biochemistry (24)Community Medicine (55)Dermatology (14)ENT (18)Forensic Medicine (17)General Medicine (2)Internal Medicine (81)Microbiology (32)Obstetrics and Gynecology (59)Ophthalmology (25)Orthopaedics (11)Pathology (44)Pediatrics (40)Pharmacology (29)Physiology (18)Psychiatry (14)Radiology (21)Surgery (44)
Q391
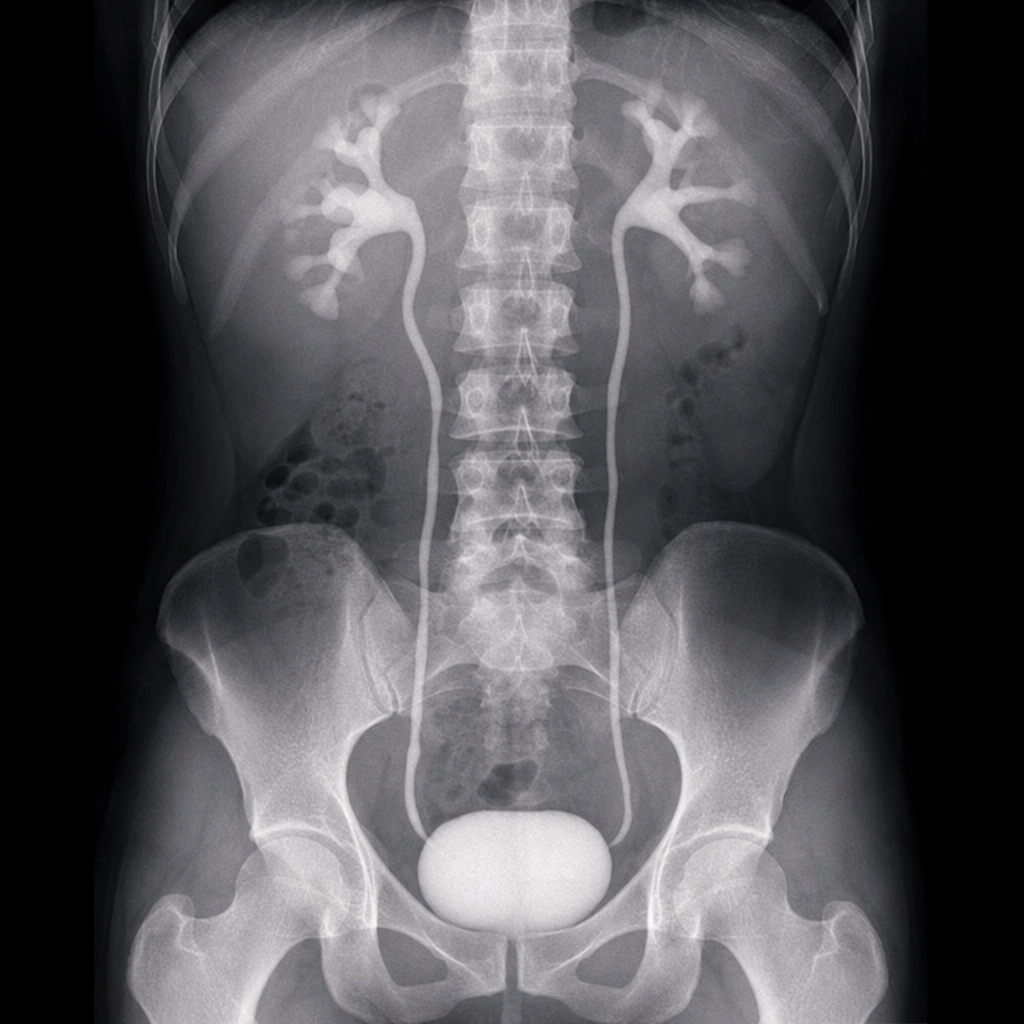
Identify the imaging study shown in the image.
Q392
A patient presents with bilateral hilar lymphadenopathy with eggshell calcification on chest X-ray. What is the most likely diagnosis?