All (607)Anatomy (42)Anesthesiology (16)Biochemistry (24)Community Medicine (55)Dermatology (14)ENT (18)Forensic Medicine (17)General Medicine (2)Internal Medicine (81)Microbiology (32)Obstetrics and Gynecology (59)Ophthalmology (25)Orthopaedics (11)Pathology (44)Pediatrics (40)Pharmacology (29)Physiology (18)Psychiatry (14)Radiology (21)Surgery (45)
Q201
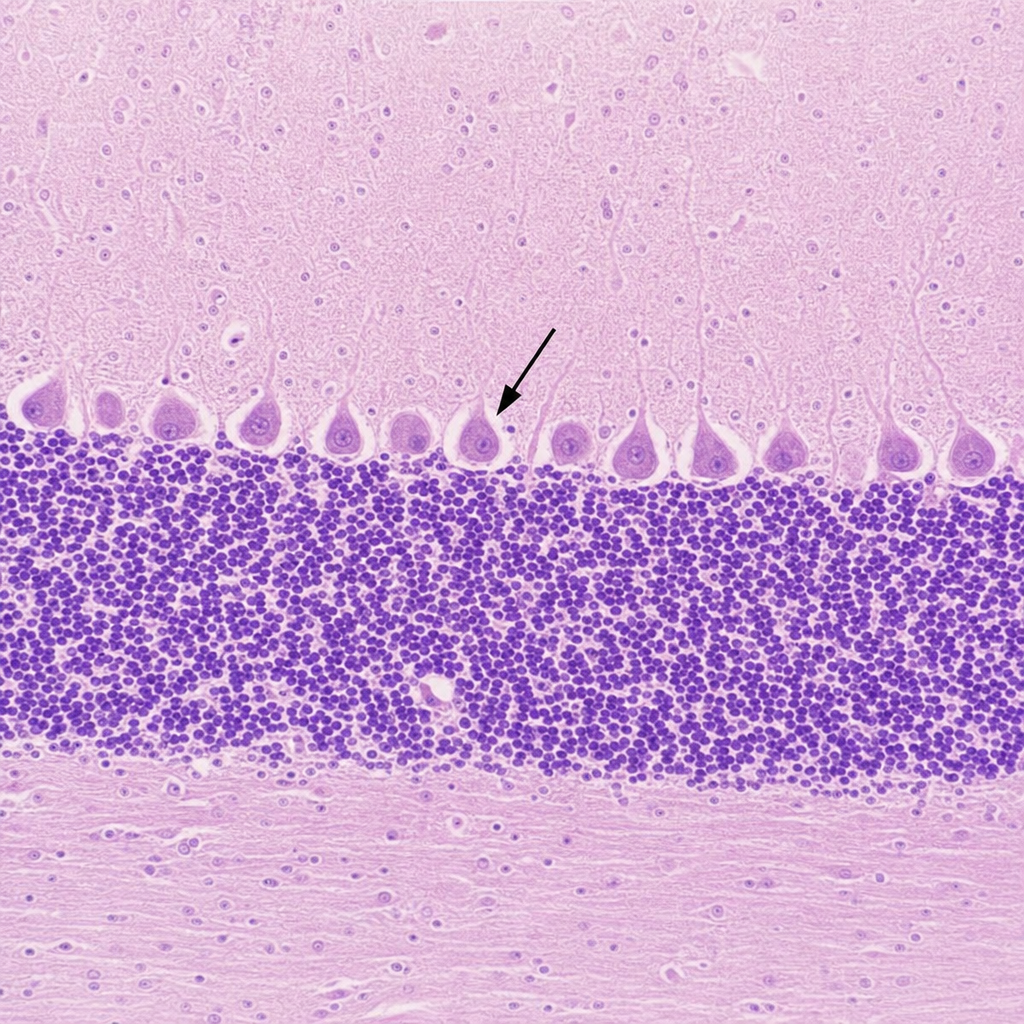
Histological section is given below. Identify the marked cell. 
Q202
Histological section is given below. Identify the marked cell.