All SubjectsAnatomy (42)Anesthesiology (16)Biochemistry (24)Community Medicine (55)Dermatology (14)ENT (18)Forensic Medicine (17)General Medicine (2)Internal Medicine (81)Microbiology (32)Obstetrics and Gynecology (59)Ophthalmology (25)Orthopaedics (11)Pathology (44)Pediatrics (40)Pharmacology (29)Physiology (18)Psychiatry (14)Radiology (21)Surgery (44)
Q11
A patient presents with eyelid crusting and a thready sensation between the cornea and lids. What is the most likely diagnosis?
Q12
A patient presents with proptosis that increases when bending down. What is the most likely diagnosis?
Q13
What is the probable diagnosis for a patient who exhibits miosis, anhidrosis, mild ptosis, and a persistent small pupil even in low light conditions?
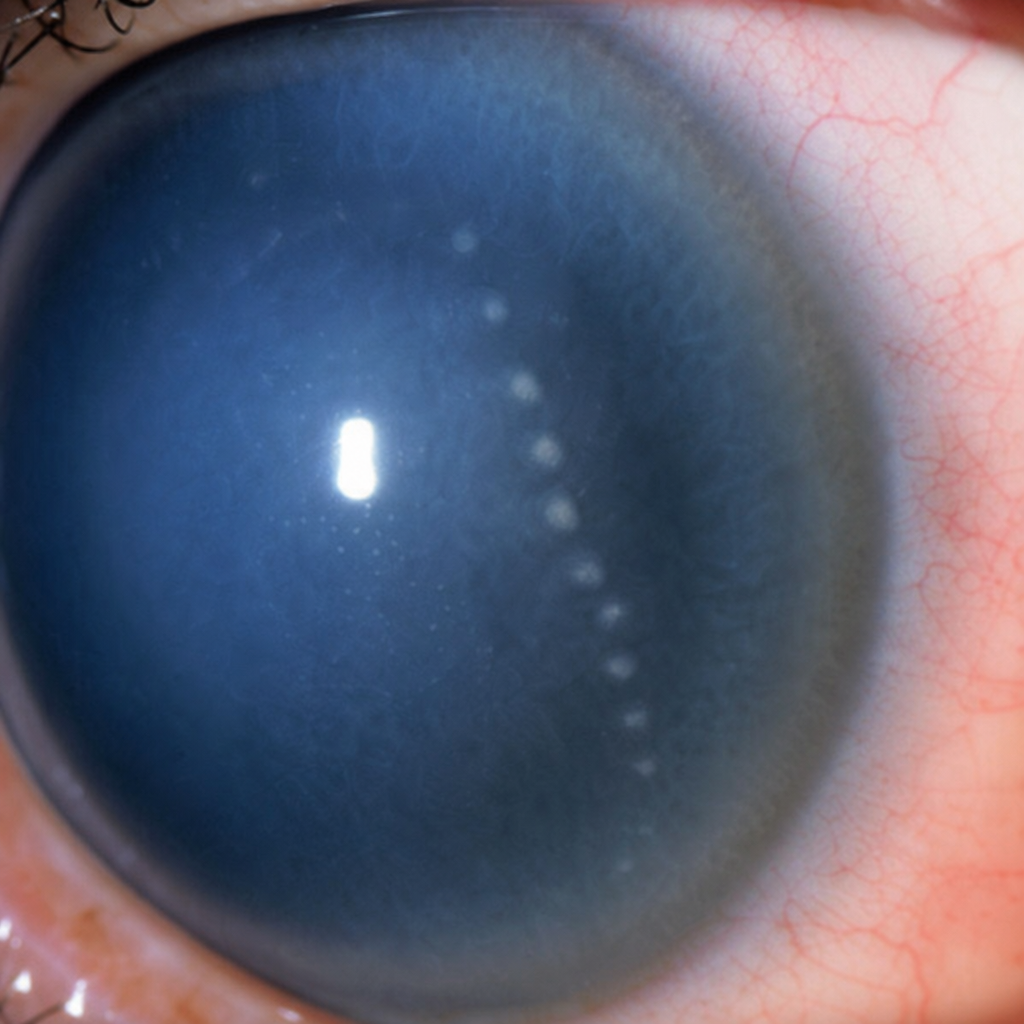
Q14
The finding seen in the image is:
Q15
A patient with pituitary adenoma compressing the optic chiasma now presents with loss of visual field. What visual field defect will be seen in the patient?
Q16
A patient presents with complaints of eye strain. The given image shows the focus of light rays in different meridians in the eye. Which refractive error is present in this patient?
Q17
A myopic patient presents with complaints of flashes and floaters. On examination, a deep anterior chamber is seen. What is the likely diagnosis?
Q18
Identify the ocular condition shown in the image.
Q19
An elderly female presents with sudden onset of pain, redness, and decreased vision. On examination, hazy cornea, fixed mid-dilated pupil, and shallow anterior chamber are noted. What is the diagnosis?
Q20
A patient presents with a painless ulcer in the eye. On examination, a long, branching ulcer with desquamated epithelium is seen on the cornea. What is the most likely diagnosis?