All SubjectsAnatomy (42)Anesthesiology (16)Biochemistry (24)Community Medicine (55)Dermatology (14)ENT (18)Forensic Medicine (17)General Medicine (2)Internal Medicine (81)Microbiology (32)Obstetrics and Gynecology (59)Ophthalmology (25)Orthopaedics (11)Pathology (44)Pediatrics (40)Pharmacology (29)Physiology (18)Psychiatry (14)Radiology (21)Surgery (45)
Q11
Identify the structure marked in the image.
Q12
A patient presents with loss of sensation on the posterior surface of the ear along with a lesion. Which structure is most likely involved?
Q13
What is the most common type of ventricular septal defect?
Q14
A corneal wisp test was performed, and the corneal reflex was elicited. Which of the following nerves is responsible for the afferent limb of this reflex?
Q15
Identify the structure marked in the image given below.
Q16
Identify the structure indicated by the arrow in the image.

Q17
Identify the marked area in the image given.
Q18
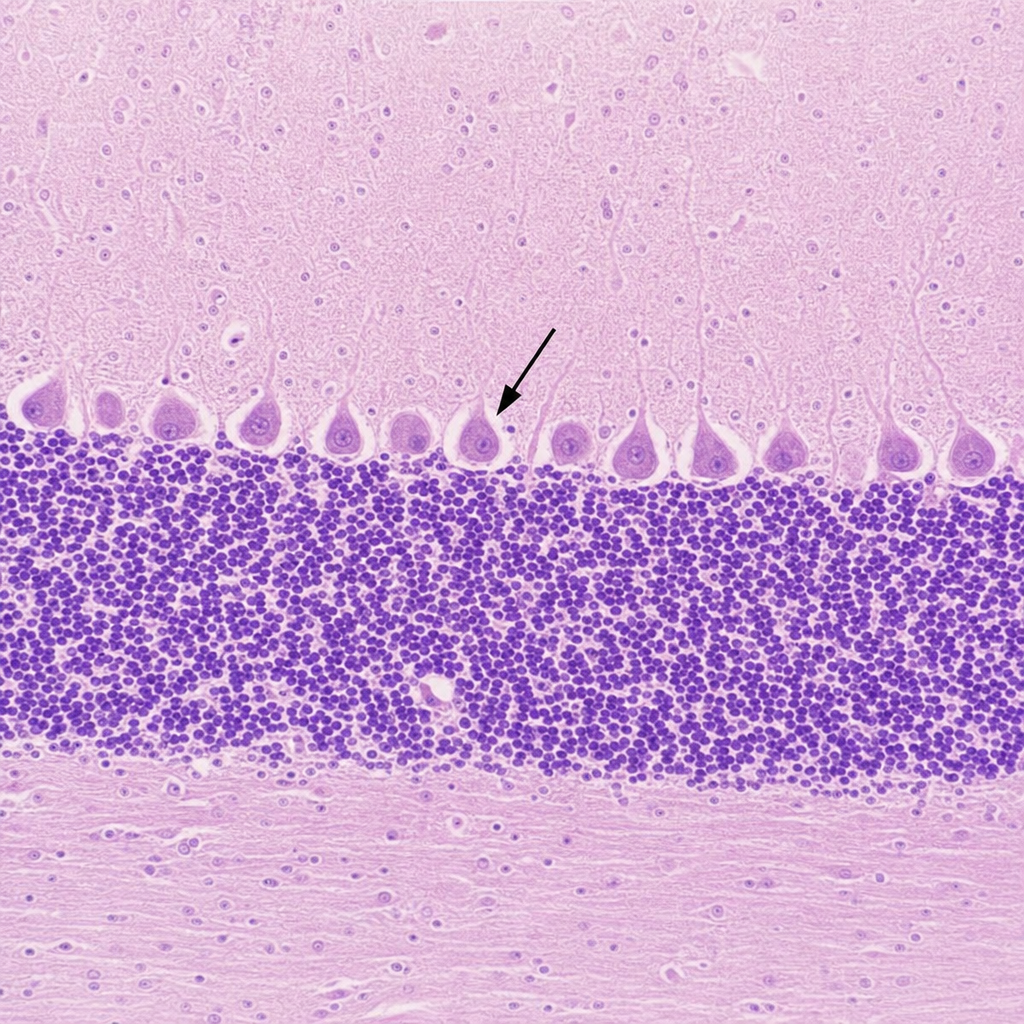
Histological section is given below. Identify the marked cell. 
Q19
Histological section is given below. Identify the marked cell.
Q20
Which nerve is affected in the hand deformity shown in the image at rest? 