All (108)Anatomy (10)Anesthesiology (4)Biochemistry (9)Community Medicine (14)Dermatology (3)ENT (4)Forensic Medicine (4)General Medicine (1)Internal Medicine (8)Microbiology (2)Obstetrics and Gynecology (5)Ophthalmology (3)Orthopaedics (3)Pathology (5)Pediatrics (8)Pharmacology (5)Physiology (5)Psychiatry (4)Radiology (6)Surgery (5)
Q51
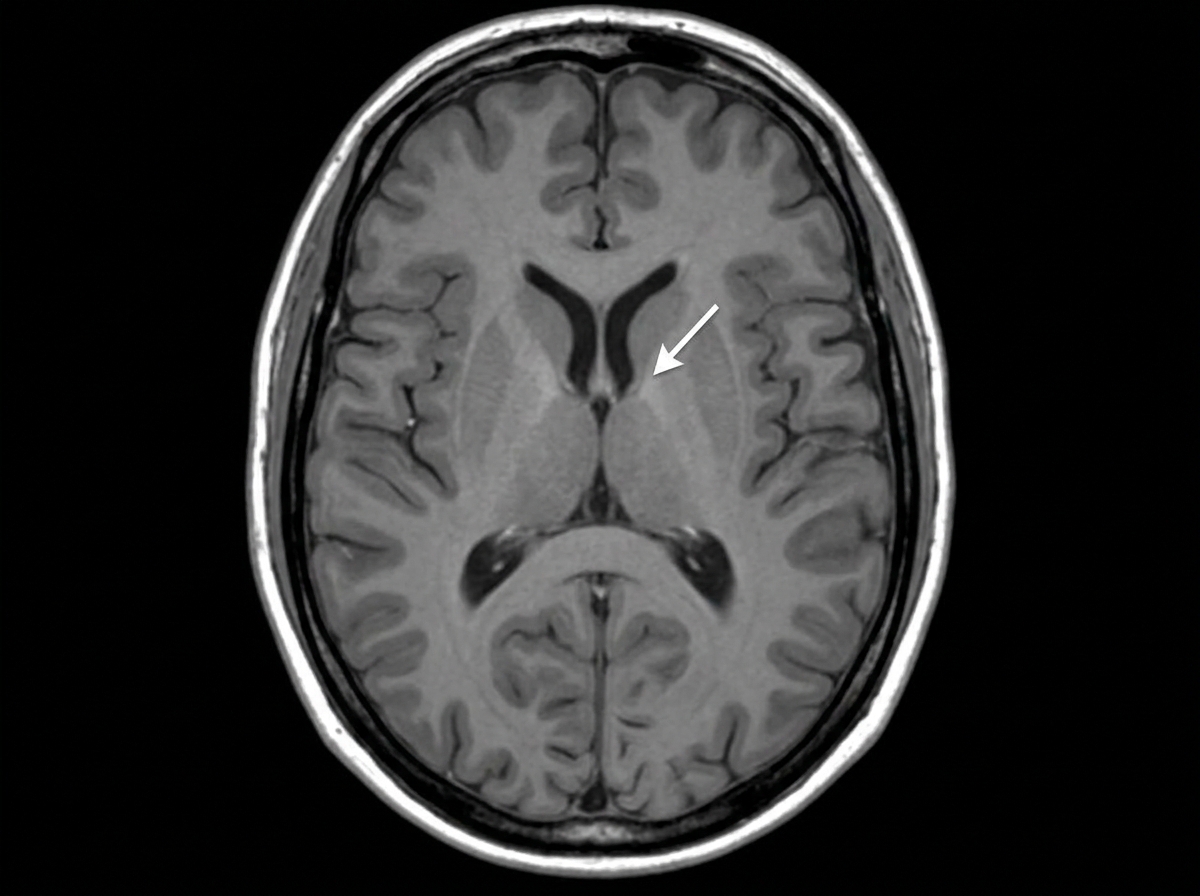
Identify the marked structure:
Q52
Which muscle is innervated by the Abducens nerve?