All SubjectsAnatomy (15)Anesthesiology (7)Biochemistry (17)Community Medicine (20)Dental (3)Dermatology (2)ENT (7)Forensic Medicine (9)Internal Medicine (36)Microbiology (23)Obstetrics and Gynecology (28)Ophthalmology (13)Orthopaedics (7)Pathology (12)Pediatrics (9)Pharmacology (27)Physiology (11)Psychiatry (7)Radiology (8)Surgery (21)
Q11
What is the most common anterior mediastinal tumor?
Q12
In an accident case, after the arrival of medical team, all should be done in early management except;
Q13
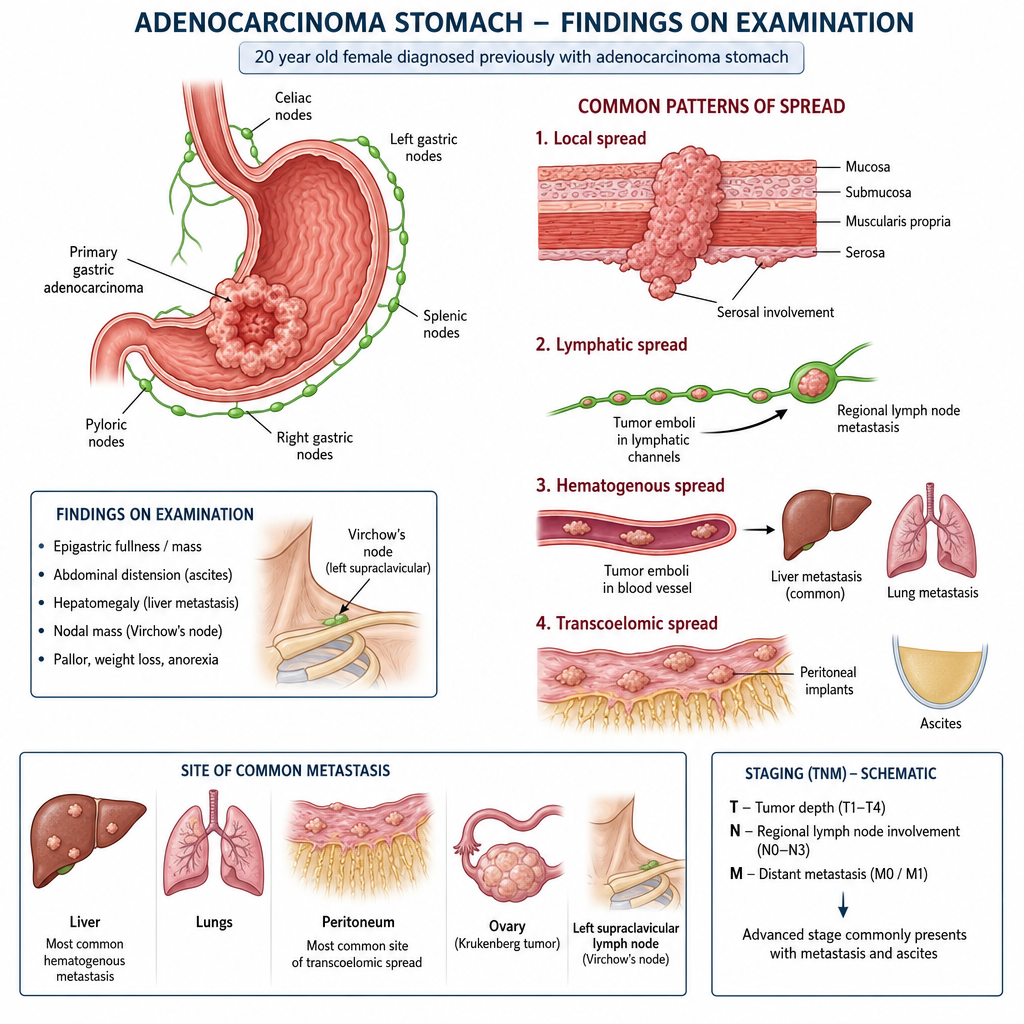
20 yr old female diagnosed previously with adenocarcinoma stomach and on examination following is seen;
Q14
In which location is a transplanted kidney typically placed?
Q15
A 27-year-old woman presents with 26 weeks of gestation with a thyroid lesion which is found to be papillary carcinoma of thyroid. Which is the best treatment for this patient?
Q16
A lady comes to OPD after fall from scooty. Her vitals are stable. She is having continuous, clear watery discharge from nose after 2 days. This is most likely a feature of?
Q17
A young male patient presents with dyspnea; auscultation reveals absent breath sounds on the right side, and he has hypotension. What is the immediate next step?
Q18
32-year-old man presented with fever and pain in upper right hypochondrium after food intake. Investigation of choice?
Q19
The complication which will not occur after PCNL surgery:
Q20
A lady with 50% TBSA burn with involvement of dermis and subcutaneous tissue came to the emergency department. The burns will be classified as: