FMGE 2019 — Radiology
6 Previous Year Questions with Answers & Explanations
A man presents to the emergency department with a head injury following a vehicular accident. What is the investigation of choice?
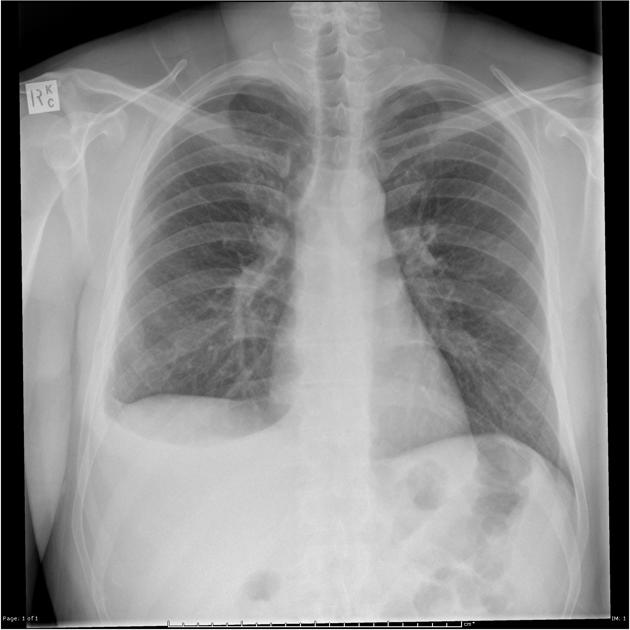
A patient presented with complaints of dyspnoea. The shown X-ray is suggestive of:
Which of the following is best assessed by FAST USG?
Which of the following typically results in the maximum radiation exposure?
Initial radiological finding seen in knee TB
PA view of chest X-ray is given here. What is the diagnosis?

FMGE 2019 - Radiology FMGE Practice Questions and MCQs
Question 1: A man presents to the emergency department with a head injury following a vehicular accident. What is the investigation of choice?
- A. MRI
- B. CECT
- C. NCCT (Correct Answer)
- D. X-ray
Explanation: ***NCCT*** - **Non-contrast Computed Tomography (NCCT)** of the head is the **investigation of choice** for acute head trauma due to its rapid acquisition, wide availability, and excellent sensitivity for detecting acute hemorrhage, fractures, and mass effects. - It rapidly identifies life-threatening conditions such as **epidural, subdural, and intracerebral hemorrhages**, which require immediate intervention. *MRI* - **MRI** is superior for detecting subtle brain tissue injuries, diffuse axonal injury, and non-hemorrhagic lesions but is generally **not the first-line investigation** in acute trauma due to longer scan times, limited availability in the emergency setting, and inability to detect acute hemorrhage as clearly as CT. - Its use is typically reserved for follow-up studies or when CT findings are inconclusive or specific soft tissue detail is required. *CECT* - **Contrast-enhanced CT (CECT)** of the head is reserved for specific indications like evaluating vascular lesions (e.g., aneurysms, arteriovenous malformations) or tumors, which are generally **not the primary concern** in the initial assessment of acute head trauma. - Administering contrast agents can delay imaging, may pose risks to patients with renal impairment or allergies, and does not significantly improve the detection of acute traumatic hemorrhage compared to NCCT. *X-ray* - **X-rays** of the skull are useful for detecting **skull fractures**, but they provide **limited information** regarding intracranial injuries or soft tissue damage, which are critical in head trauma. - They have largely been superseded by CT scans, which offer a more comprehensive view of both bony structures and intracranial contents.
Question 2: A patient presented with complaints of dyspnoea. The shown X-ray is suggestive of:
- A. Pleural effusion (Correct Answer)
- B. Pneumothorax
- C. Hydropneumothorax
- D. Consolidation
Explanation: ***Pleural effusion*** - The X-ray shows a significant **right-sided pleural effusion** with blunting of the costophrenic angle and a meniscus sign characteristic of fluid accumulation in the pleural space. - Key radiological features include: **homogeneous opacity** in the lower zone, **obliteration of the costophrenic angle**, and the typical **concave upper border (meniscus sign)** of fluid layering. - The presence of dyspnea with these radiological findings is consistent with pleural effusion. **Note:** While the X-ray confirms pleural effusion, **differentiating between exudative and transudative effusion requires pleural fluid analysis** (Light's criteria), not imaging alone. *Pneumothorax* - A pneumothorax would appear as a **dark, air-filled space** with a visible **visceral pleural line** where the lung has collapsed away from the chest wall. - The image clearly shows **fluid opacity** (white/grey) in the right hemithorax, not air (black). *Hydropneumothorax* - This condition involves both **fluid and air** in the pleural space, typically presenting with a **straight horizontal air-fluid level** on an erect chest X-ray. - The X-ray here shows a **curved meniscus** rather than a straight air-fluid level, indicating pure fluid without air. *Consolidation* - Consolidation (as seen in pneumonia) appears as a **homogenous opacity within the lung parenchyma**, often with **air bronchograms**. - The image shows fluid in the **pleural space** (outside the lung), **displacing the lung medially**, rather than an opacity within the lung tissue itself.
Question 3: Which of the following is best assessed by FAST USG?
- A. Liver
- B. Pericardium (Correct Answer)
- C. Spleen
- D. Pleural cavity
Explanation: ***Pericardium*** - FAST USG is **most clinically significant** for detecting **pericardial effusions** and **cardiac tamponade** in trauma patients. - The **subxiphoid view** provides **excellent direct visualization** of the heart and pericardial space with minimal interference. - **Small volumes** of pericardial fluid (as little as 50-100 mL) are **clinically significant** and potentially life-threatening, requiring immediate intervention. - Cardiac tamponade is an **immediately reversible cause of shock** that demands urgent diagnosis and pericardiocentesis. - **Sensitivity >90%** for clinically significant pericardial effusions in the trauma setting. *Liver* - FAST assesses the **hepatorenal space (Morison's pouch)** for free fluid, not the liver parenchyma itself. - Requires **larger volumes of free fluid** (>200-500 mL) to be reliably detected in the peritoneal cavity. - Detailed assessment of actual liver injury requires **contrast-enhanced CT imaging**. *Spleen* - FAST evaluates the **splenorenal recess** for free fluid surrounding the spleen, not splenic parenchymal injury. - Detection depends on adequate volume of free fluid being present. - **CT scanning** is superior for defining splenic lacerations, hematomas, and grading injury severity. *Pleural cavity* - While Extended FAST (eFAST) can assess **pleural spaces** for effusion or pneumothorax, this is an **extension** of the standard 4-view FAST protocol. - Standard FAST focuses on the **four primary windows**: pericardial, perihepatic, perisplenic, and pelvic. - **Chest X-ray** and **CT** remain primary modalities for comprehensive thoracic assessment.
Question 4: Which of the following typically results in the maximum radiation exposure?
- A. Chest X ray
- B. IV pyelography
- C. PET CT (Correct Answer)
- D. Barium Enema
- E. X-ray abdomen
Explanation: ***PET CT*** - **PET CT (Positron Emission Tomography-Computed Tomography)** combines the radiation from both a PET scan (using radiotracers like FDG) and a CT scan, resulting in the highest typical radiation exposure among the listed options. - The integration of functional (PET) and anatomical (CT) imaging, while providing comprehensive diagnostic information, significantly increases the total absorbed dose (~20-30 mSv). *Chest X-ray* - A **chest X-ray** involves a very low dose of radiation (~0.1 mSv), making it one of the imaging modalities with the least radiation exposure. - Due to its low dose and widespread use, the benefits of chest X-rays in diagnosing pulmonary and cardiac conditions far outweigh the minimal radiation risk. *IV pyelography* - **Intravenous pyelography (IVP)**, or intravenous urography, uses X-rays and contrast dye to visualize the urinary tract, delivering a moderate radiation dose (~3-5 mSv). - While higher than a standard X-ray, its dose is significantly lower than that of complex combined imaging like PET-CT. *Barium Enema* - A **barium enema** involves multiple X-ray images of the large intestine after administering barium contrast, leading to a moderate to high radiation dose (~8-15 mSv). - The series of exposures required to adequately visualize the entire colon contributes to a higher cumulative dose compared to single-shot X-rays.
Question 5: Initial radiological finding seen in knee TB
- A. Reduction of joint space
- B. Bone resorption
- C. Increase in joint space (Correct Answer)
- D. Degeneration of cartilage
Explanation: ***Increase in joint space*** - Early **tuberculous synovitis** leads to synovial hypertrophy and effusion, causing an **increase in joint space** due to fluid accumulation on imaging. - This is the **initial radiological finding** before significant cartilage destruction or bone erosion occurs. - Part of **Phemister's triad** (juxta-articular osteoporosis, peripheral erosions, and gradual joint space reduction in later stages). *Reduction of joint space* - **Joint space narrowing** typically occurs later in the disease as the **cartilage is destroyed**. - This finding is more characteristic of advanced tuberculous arthritis, not the initial stages of knee TB. *Bone resorption* - **Bone resorption (osteolysis)** is a later manifestation of knee TB, often seen with **caseous necrosis** and subchondral bone involvement. - It does not represent the very initial radiological changes, which are primarily synovial-based. *Degeneration of cartilage* - While cartilage is eventually affected by knee TB, **cartilage degeneration** leading to significant changes visualized on imaging is a later event. - The initial presentation is more about synovial inflammation and fluid buildup causing increased joint space.
Question 6: PA view of chest X-ray is given here. What is the diagnosis?
- A. Right Pneumothorax with left tracheal shift (Correct Answer)
- B. Left Pneumothorax with right tracheal shift
- C. Left Pneumothorax with left tracheal shift
- D. Right Pneumothorax with right tracheal shift
Explanation: ***Right Pneumothorax with left tracheal shift*** - The image shows a large **radiolucency (black area) on the right side** of the chest, indicative of **air in the pleural space**, consistent with a **right-sided pneumothorax**. - The **trachea is shifted towards the left** (away from the pneumothorax), which is the **expected finding** in pneumothorax due to increased pressure in the right pleural space pushing mediastinal structures to the contralateral side. - In pneumothorax, the trachea and mediastinum shift **away from** the affected side due to the pressure effect of air accumulation in the pleural cavity. - This **contralateral tracheal deviation** is a classic radiological sign of pneumothorax and helps confirm the diagnosis. *Right Pneumothorax with right tracheal shift* - While the **right pneumothorax** is correctly identified, the tracheal shift direction is incorrect. - In pneumothorax, the trachea shifts **away from** the affected side (contralateral), not toward it (ipsilateral). - **Ipsilateral tracheal shift** would suggest volume loss (atelectasis) or lung collapse, not pneumothorax alone. *Left Pneumothorax with right tracheal shift* - The pneumothorax is clearly on the **right side**, not the left. - The radiolucency and absent lung markings are visible on the right hemithorax. - A left pneumothorax would show these findings on the left side. *Left Pneumothorax with left tracheal shift* - There is **no pneumothorax on the left side** of the chest. - The left lung shows normal vascular markings and no evidence of pleural air. - This combination would be medically implausible as it suggests pneumothorax with ipsilateral shift.