FMGE 2019 — Physiology
10 Previous Year Questions with Answers & Explanations
What is the principal stimulus for vasopressin secretion?
NaCl symporter is present in which part of the nephron?
Which of the following causes hypoxic hypoxia?
Secretion of prolactin is inhibited by?
Which of the following has prolonged inspiratory spasms that resemble breath holding?
Testosterone is secreted by:
PR interval in ECG shows?
In this normal menstrual cycle graph, the mark 'X' represents levels of which hormone?
Normal anion gap is___ mmol/L?
Which muscle tendon is stretched in patellar tendon reflex?
FMGE 2019 - Physiology FMGE Practice Questions and MCQs
Question 1: What is the principal stimulus for vasopressin secretion?
- A. Hyperosmolality (Correct Answer)
- B. Hypovolemia
- C. Hypoosmolality
- D. Hypervolemia
Explanation: ***Hyperosmolality*** - An increase in **plasma osmolality**, even by a small percentage (1-2%), is the **most potent and PRINCIPAL stimulus** for ADH (vasopressin) release. - This is detected by **osmoreceptors** in the hypothalamus (particularly in the organum vasculosum of the lamina terminalis), which are extremely sensitive and respond rapidly. - This response is the primary mechanism for day-to-day regulation of water balance. *Hypovolemia* - A significant decrease in **blood volume** (typically >10%) also stimulates vasopressin release, but it is **much less sensitive** than hyperosmolality and serves as a secondary/backup mechanism. - This response is mediated by **baroreceptors** in the carotid sinuses and aortic arch. - Only activated during substantial volume loss (hemorrhage, severe dehydration). *Hypoosmolality* - **Decreased plasma osmolality** actively **inhibits** vasopressin secretion as the body aims to excrete excess water. - This helps to prevent overhydration and maintain proper fluid balance. *Hypervolemia* - **Increased blood volume** (hypervolemia) **inhibits** vasopressin secretion, as the body needs to excrete excess fluid. - This contributes to diuresis and the lowering of blood pressure.
Question 2: NaCl symporter is present in which part of the nephron?
- A. PCT
- B. DCT (Correct Answer)
- C. Loop of Henle
- D. Collecting duct
Explanation: ***DCT*** - The **NaCl symporter** (also known as the **Na-Cl co-transporter** or NCC) is located in the **luminal membrane** of cells in the **distal convoluted tubule (DCT)**. - This transporter is responsible for reabsorbing approximately 5-10% of filtered sodium and chloride, and it is the target of **thiazide diuretics**. *PCT* - The **proximal convoluted tubule (PCT)** is responsible for bulk reabsorption of Na+ through various mechanisms, including Na+/H+ exchangers and Na+-glucose co-transporters, but not the specific NaCl symporter found in the DCT. - While significant NaCl reabsorption occurs here, it is primarily driven by different transport proteins. *Loop of Henle* - The **thick ascending limb of the loop of Henle** uses the **Na-K-2Cl co-transporter (NKCC2)** for Na+ reabsorption, which is distinct from the NaCl symporter. - This segment is the target for **loop diuretics**. *Collecting duct* - The **collecting duct** reabsorbs Na+ primarily through the **epithelial sodium channel (ENaC)**, which is regulated by aldosterone. - While reabsorption of sodium occurs, the specific NaCl symporter is not present in this segment.
Question 3: Which of the following causes hypoxic hypoxia?
- A. Pneumonia (Correct Answer)
- B. HCN poisoning
- C. CO poisoning
- D. Circulatory shock
Explanation: ***Pneumonia*** - Pneumonia causes **hypoxic hypoxia** by impairing **gas exchange** in the lungs due to inflammation and fluid accumulation in the alveoli, leading to reduced oxygen uptake. - This results in a **low partial pressure of oxygen (PaO2)** in the arterial blood, even with normal oxygen-carrying capacity and tissue perfusion. *HCN poisoning* - **Hydrogen cyanide (HCN) poisoning** causes **histotoxic hypoxia**, where cells are unable to utilize oxygen despite adequate delivery, by inhibiting **cytochrome c oxidase** in the electron transport chain. - It does not directly reduce the amount of oxygen in the blood or its delivery to tissues. *CO poisoning* - **Carbon monoxide (CO) poisoning** causes **anemic hypoxia** by binding to hemoglobin with a much higher affinity than oxygen, forming **carboxyhemoglobin (COHb)**. - This reduces the **oxygen-carrying capacity** of the blood and shifts the oxygen-hemoglobin dissociation curve to the left, but it is not a direct problem with alveolar gas exchange or oxygen partial pressure. *Circulatory shock* - **Circulatory shock** causes **stagnant or ischemic hypoxia**, characterized by reduced blood flow and oxygen delivery to tissues due to systemic circulatory failure. - While it results in tissue oxygen deprivation, the primary issue is impaired perfusion rather than a defect in the initial oxygenation of blood in the lungs or the blood's capacity to carry oxygen.
Question 4: Secretion of prolactin is inhibited by?
- A. Dopamine (Correct Answer)
- B. Serotonin
- C. Noradrenaline
- D. Adrenaline
Explanation: ***Dopamine*** - **Dopamine**, produced by the **hypothalamus**, is the primary physiological inhibitor of **prolactin secretion** from the anterior pituitary gland. - It acts on **D2 receptors** on lactotrophs, leading to a decrease in prolactin synthesis and release. *Serotonin* - **Serotonin** generally has a stimulatory effect on **prolactin secretion**, rather than an inhibitory one. - Elevated serotonin levels can lead to **hyperprolactinemia**. *Noradrenaline* - While **noradrenaline** can have complex effects on pituitary hormones, it is not considered the primary direct inhibitor of **prolactin secretion**. - Its influence is often indirect or less potent than that of **dopamine**. *Adrenaline* - **Adrenaline** (epinephrine) is a neurotransmitter and hormone primarily involved in the **"fight or flight" response** and does not directly inhibit **prolactin secretion**. - Its effects on pituitary hormone release are typically less direct compared to **dopamine's** specific action on lactotrophs.
Question 5: Which of the following has prolonged inspiratory spasms that resemble breath holding?
- A. Kussmaul breathing
- B. Biot breathing
- C. Apneustic breathing (Correct Answer)
- D. Cheyne-Stokes breathing
Explanation: ***Apneustic breathing*** - This pattern is characterized by **prolonged inspiratory pauses**, resembling breath-holding, followed by a short, insufficient expiratory phase. - It is caused by damage to the **pons** in the brainstem, often due to stroke or trauma, which disrupts the normal rhythm of breathing. *Kussmaul breathing* - Characterized by **deep**, **rapid**, and labored breathing, typically seen in metabolic acidosis like **diabetic ketoacidosis**. - It is a compensatory mechanism to increase CO2 elimination and raise blood pH. *Biot's breathing* - Involves irregular breathing with **periods of apnea** interspersed with shallow breaths. - This pattern is associated with damage to the **medulla oblongata** or severe intracranial pressure. *Cheyne-Stokes breathing* - Characterized by a **crescendo-decrescendo pattern** of respiration, where breathing gradually increases in depth and rate, then decreases, followed by a period of **apnea**. - It is often observed in **heart failure**, stroke, or severe neurological conditions, indicating brainstem or cerebral dysfunction.
Question 6: Testosterone is secreted by:
- A. Leydig cell (Correct Answer)
- B. Granulosa cell
- C. Theca cells
- D. Sertoli cell
Explanation: ***Leydig cell*** - **Leydig cells** are located in the **interstitial tissue** of the testes and are responsible for producing **testosterone** in response to **luteinizing hormone (LH)** stimulation. - They are the primary source of androgens in males, crucial for the development of male secondary sexual characteristics and spermatogenesis. *Granulosa cell* - **Granulosa cells** are found in the **ovarian follicles** and are primarily involved in the production of **estrogen** and **progesterone** in females. - They surround the oocyte and convert androgens (produced by theca cells) into estrogens. *Theca cells* - **Theca cells** are found in the **ovarian follicles** and produce **androgens** (mainly androstenedione) in response to **LH** stimulation. - These androgens are then converted to estrogens by the adjacent granulosa cells through aromatization. - While they produce androgens, they are not the primary source of testosterone in the body. *Sertoli cell* - **Sertoli cells** are located in the **seminiferous tubules** of the testes and provide structural and metabolic support for **spermatogenesis**. - They produce substances like **androgen-binding protein**, inhibin, and Müllerian inhibiting factor, but they do not secrete testosterone.
Question 7: PR interval in ECG shows?
- A. Atrial depolarization and conduction delay (Correct Answer)
- B. Conduction through AV node
- C. Delay in ventricular depolarization
- D. Delay in ventricular repolarization
Explanation: ***Atrial depolarization and conduction delay*** - The **PR interval** is measured from the **beginning of the P wave** to the **beginning of the QRS complex**. - It represents the **complete time** for the electrical impulse to travel from the SA node through the atria, the AV node, the Bundle of His, and bundle branches until ventricular depolarization begins. - This includes two major components: 1. **Atrial depolarization** (represented by the P wave) 2. **Conduction delay** through the AV node and His-Purkinje system (the isoelectric segment after the P wave) - **Normal PR interval**: 0.12-0.20 seconds (120-200 ms) - The **AV nodal delay** is the longest component, allowing atrial contraction to complete before ventricular contraction begins. *Conduction through AV node* - While **AV nodal conduction** is an important component of the PR interval, this option is **incomplete**. - The PR interval begins with the **P wave** (atrial depolarization), which occurs before the impulse reaches the AV node. - Stating only "conduction through AV node" ignores the atrial depolarization component that is also part of the PR interval. *Delay in ventricular depolarization* - **Ventricular depolarization** is represented by the **QRS complex**, not the PR interval. - The PR interval *ends* when ventricular depolarization begins (start of QRS). *Delay in ventricular repolarization* - **Ventricular repolarization** is represented by the **T wave** on an ECG. - This occurs much later in the cardiac cycle and is not related to the PR interval.
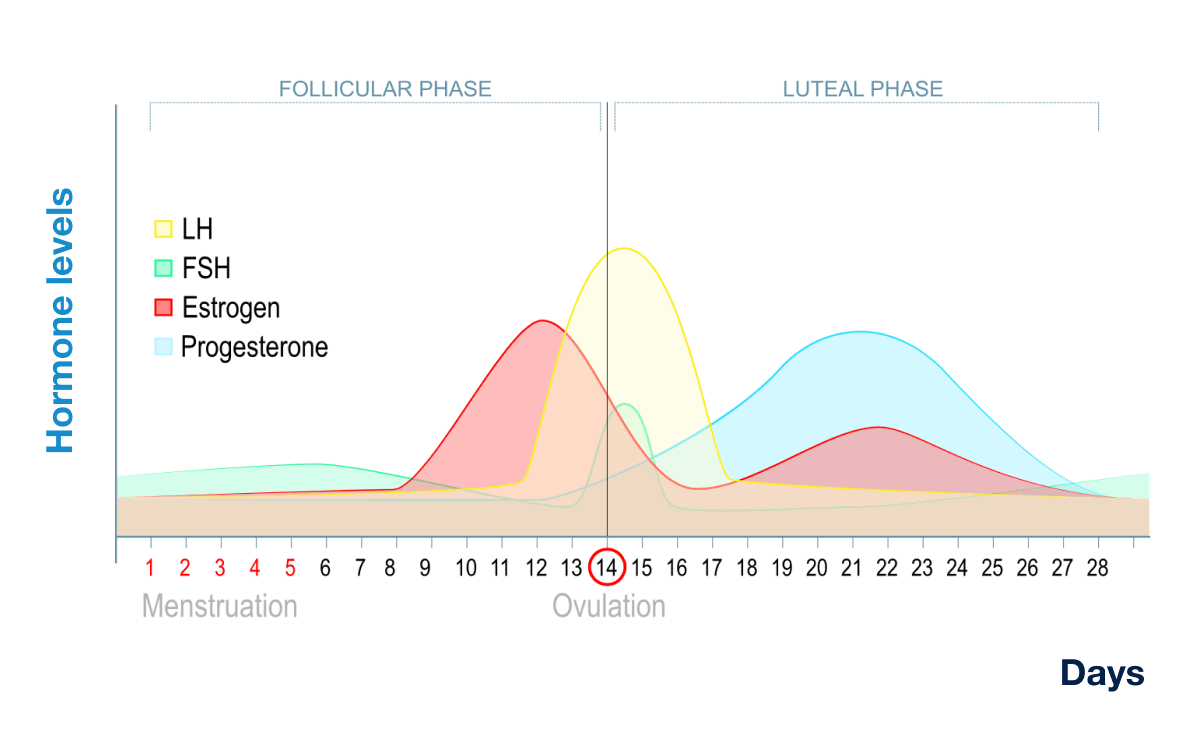
Question 8: In this normal menstrual cycle graph, the mark 'X' represents levels of which hormone?
- A. LH
- B. FSH
- C. Progesterone (Correct Answer)
- D. Estrogen
Explanation: ***Progesterone*** - The mark 'X' (blue line) represents a hormone that significantly rises during the **luteal phase** after ovulation, reaching its peak around day 21-24 and then declining if pregnancy does not occur. - This pattern is characteristic of **progesterone**, which is primarily produced by the corpus luteum after ovulation to prepare the uterus for potential implantation. *LH* - **Luteinizing Hormone (LH)** is characterized by a sharp, transient peak just before ovulation (around day 14), which triggers the release of the egg. The blue line does not show this pre-ovulatory surge. - After ovulation, LH levels generally fall and remain relatively low throughout the luteal phase, unlike the sustained high levels shown by the blue line. *FSH* - **Follicle-Stimulating Hormone (FSH)** levels are typically higher during the early follicular phase, promoting follicle growth, and then decrease as estrogen rises. There is a smaller, transient peak around ovulation. - The blue line's profile, with its primary peak in the mid-luteal phase, does not match the typical FSH secretion pattern. *Estrogen* - **Estrogen** (specifically estradiol) typically shows a prominent peak during the late follicular phase, preceding the LH surge, and a secondary, smaller peak in the mid-luteal phase. - The blue line's peak is much higher and more sustained during the luteal phase than expected for estrogen, which is usually represented by the red curve in such graphs.
Question 9: Normal anion gap is___ mmol/L?
- A. 8-16 (Correct Answer)
- B. 30-34
- C. 20-24
- D. 0-4
Explanation: ***8-16*** - The normal range for the **anion gap** is generally considered to be 8-16 mmol/L, reflecting the unmeasured anions in the plasma. - This range can vary slightly between laboratories, but **8-16 mmol/L** is the most commonly accepted range in clinical practice. *30-34* - This range is significantly **higher than normal** and would indicate a **high anion gap metabolic acidosis**, rather than a normal anion gap. - A high anion gap suggests an accumulation of **unmeasured acids** in the body, such as in lactic acidosis or ketoacidosis. *20-24* - This value is also **elevated** compared to the normal range, suggesting a high anion gap. - An anion gap in this range would prompt investigation into causes of **metabolic acidosis** with an increased anion gap. *0-4* - This range is significantly **lower than normal** and could indicate a **low or negative anion gap**, which is a rare finding. - A low anion gap is often associated with conditions like **hypoalbuminemia**, multiple myeloma (due to paraproteins), or severe hypernatremia.
Question 10: Which muscle tendon is stretched in patellar tendon reflex?
- A. Biceps femoris
- B. Semitendinosus
- C. Quadriceps femoris (Correct Answer)
- D. Adductor magnus
Explanation: ***Quadriceps femoris*** - The patellar tendon reflex is an example of a **stretch reflex**, where striking the patellar tendon directly stretches the quadriceps femoris muscle. - This stretch activates **muscle spindles** within the quadriceps, leading to its contraction and subsequent leg extension. *Biceps femoris* - The biceps femoris is part of the **hamstring muscle group**, located on the posterior aspect of the thigh. - Its primary action is **knee flexion** and hip extension, and it is not directly stretched during the patellar tendon reflex. *Semitendinosus* - The semitendinosus is also a **hamstring muscle** and functions in knee flexion and hip extension. - It is located medially on the posterior thigh and is not involved in the patellar tendon reflex arc. *Adductor magnus* - The adductor magnus is a large muscle on the **medial side of the thigh**, primarily responsible for **hip adduction**. - It is not directly stretched by tapping the patellar tendon and does not participate in the patellar reflex.