All (281)Anatomy (15)Anesthesiology (7)Biochemistry (17)Community Medicine (19)Dental (3)Dermatology (2)ENT (7)Forensic Medicine (9)Internal Medicine (36)Microbiology (23)Obstetrics and Gynecology (28)Ophthalmology (13)Orthopaedics (7)Pathology (12)Pediatrics (9)Pharmacology (27)Physiology (11)Psychiatry (7)Radiology (8)Surgery (21)
Q171
Testicular artery is a branch of -
Q172
Trigone of bladder is derived from?
Q173
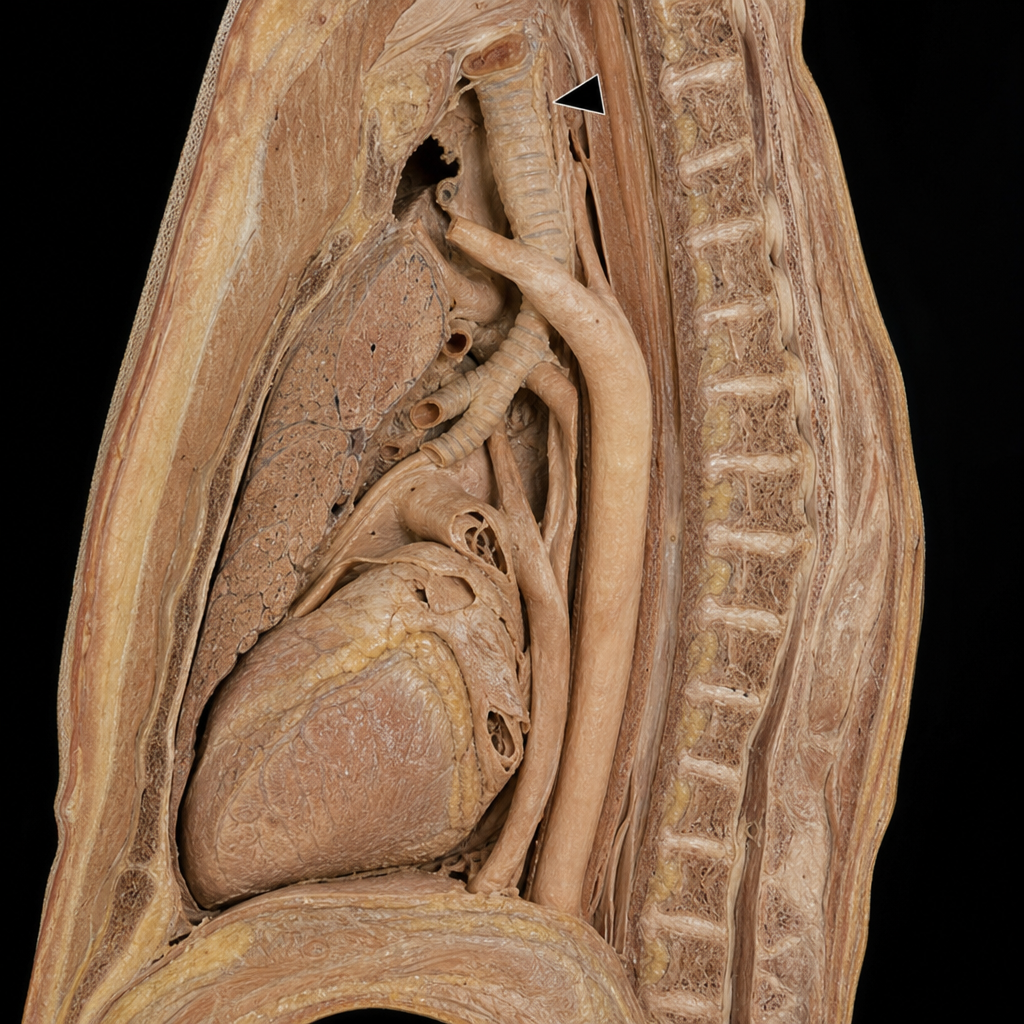
In the shown lateral view, the structure marked with arrowhead is?