

Acute Pericarditis - Sac on Fire
- Etiology: Most commonly idiopathic (presumed viral). Other causes include autoimmune disease (e.g., SLE), uremia, post-myocardial infarction (Dressler syndrome), and trauma.
- Clinical Presentation:
- Chest Pain: Sudden, sharp, pleuritic, and retrosternal. Classically improves with sitting up and leaning forward, worsens when supine.
- Pericardial Friction Rub: High-pitched, scratching, or grating sound best heard at the left sternal border.
- ECG Findings:
- Diffuse, concave ST-segment elevation across multiple leads.
- PR-segment depression (highly specific).
⭐ Exam Favorite: Unlike the localized ST elevation seen in myocardial infarction, the ST elevation in acute pericarditis is diffuse, involving nearly all leads except aVR and V1.
- Treatment: NSAIDs (e.g., ibuprofen, indomethacin) and colchicine are first-line. Corticosteroids are reserved for refractory or autoimmune cases.
Pericardial Effusion & Tamponade - Water Torture
- Pericardial Effusion: Excess fluid in the pericardial sac. Can be serous, serosanguinous, or purulent.
- Etiologies: Idiopathic (viral), infection (TB), malignancy, uremia, autoimmune, post-MI (Dressler syndrome).
- Cardiac Tamponade: Effusion that impairs cardiac filling, leading to ↓ cardiac output & shock. The rate of fluid accumulation is more critical than the volume.
- Clinical Presentation (Tamponade):
- Beck's Triad (📌 Big Effusion Compresses K): BP low (Hypotension), Elevated JVP, Cannot hear heart (Muffled sounds).
- Pulsus Paradoxus: Inspiratory SBP drop >10 mmHg.
- Tachycardia, dyspnea, shock.
- Diagnostics:
- ECG: Low-voltage QRS, electrical alternans (swinging heart).
- CXR: Globular, "water-bottle" heart silhouette.
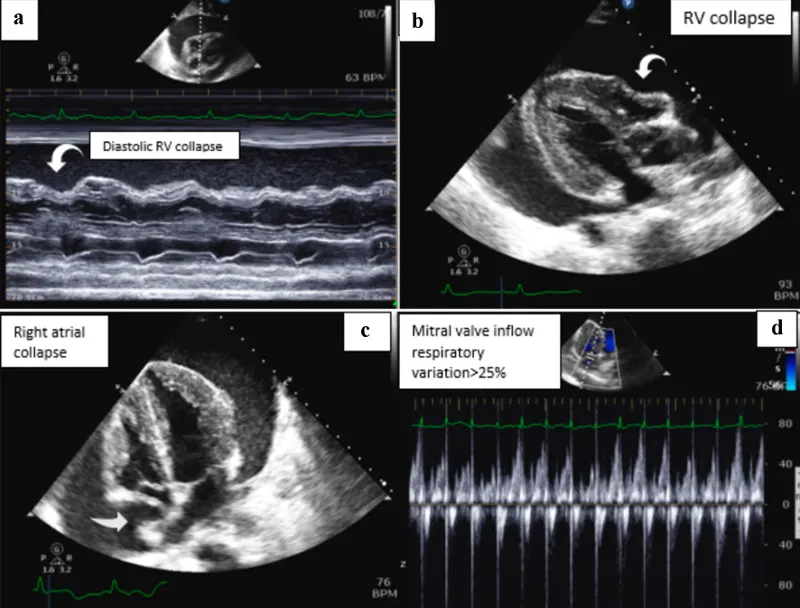
⭐ Echocardiography is the gold standard, revealing effusion size and diastolic collapse of the right atrium/ventricle-the most specific sign of tamponade.
- Management: Urgent pericardiocentesis or pericardial window.
Constrictive Pericarditis - The Unyielding Cage
- Pathophysiology: A thickened, fibrotic, and often calcified pericardium encases the heart, severely limiting diastolic filling. This leads to fixed cardiac output and signs of right-sided heart failure.
- Etiologies: Most commonly idiopathic or post-viral. Can also result from cardiac surgery, radiation therapy, or tuberculosis.
- Clinical Signs:
- Kussmaul's sign: Paradoxical ↑ in JVP on inspiration.
- Pericardial knock: An early, high-pitched diastolic sound.
- Prominent y descent (Friedreich's sign) in JVP.

⭐ Hemodynamic Hallmark: Equalization of diastolic pressures in all four cardiac chambers, producing the characteristic "square root sign" or "dip-and-plateau" waveform on right heart catheterization.
- Management: Definitive treatment is surgical pericardiectomy.
- Acute pericarditis presents with pleuritic chest pain relieved by leaning forward, a pathognomonic friction rub, and diffuse ST-segment elevation.
- Cardiac tamponade is a medical emergency characterized by Beck's triad (hypotension, JVD, muffled heart sounds) and pulsus paradoxus.
- Constrictive pericarditis shows a pericardial knock on auscultation and Kussmaul's sign (paradoxical rise in JVP with inspiration).
- Dressler syndrome is a delayed form of pericarditis occurring weeks to months after a myocardial infarction.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more