Cryptococcosis Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Cryptococcosis. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Cryptococcosis Indian Medical PG Question 1: Which of the following is NOT a virulence factor of Cryptococcus?
- A. Polysaccharide capsule
- B. Ability to make melanin
- C. Production of protease (Correct Answer)
- D. Urease production
Cryptococcosis Explanation: ***Production of protease***
- While *Cryptococcus neoformans* can produce some proteolytic enzymes, **protease production is not considered a major or classical virulence factor** in standard medical microbiology literature.
- Unlike the other three factors listed, proteases are not prominently featured as key virulence mechanisms in *Cryptococcus* pathogenesis for medical education purposes.
- The primary virulence factors emphasized for *Cryptococcus* are the capsule, melanin, and urease.
*Polysaccharide capsule*
- The **polysaccharide capsule** is the MOST important virulence factor, protecting the yeast from phagocytosis and immune clearance.
- It interferes with antigen presentation, antibody binding, and complement activation, making it crucial for survival in the host.
*Ability to make melanin*
- **Melanin production** protects *Cryptococcus* from oxidative stress, free radicals, UV radiation, and antifungal agents.
- It contributes to survival in macrophages and persistence in the central nervous system.
*Urease production*
- **Urease production** enables *Cryptococcus* to cross the blood-brain barrier and colonize the central nervous system.
- Urease hydrolyzes urea into ammonia, causing local alkalinization that facilitates CNS invasion and contributes to meningoencephalitis.
Cryptococcosis Indian Medical PG Question 2: Most serious characteristic finding of HIV in children is?
- A. Kaposi sarcoma is common
- B. Cryptococcal diarrhoea is common
- C. Recurrent chest infection (Correct Answer)
- D. Recurrent candidiasis
Cryptococcosis Explanation: ***Recurrent chest infection***
- **Recurrent chest infections**, particularly with common bacterial pathogens, are a hallmark of HIV in children due to their underdeveloped immune systems being further compromised.
- Children with HIV are highly susceptible to respiratory infections such as **pneumonia** and **bronchiolitis**, leading to frequent hospitalizations and poor outcomes.
*Kaposi sarcoma is common*
- **Kaposi sarcoma** is a well-known HIV-associated malignancy, but it is much more prevalent in **HIV-positive adults**, especially men who have sex with men, rather than in children.
- While it can occur in children, it is not considered a *characteristic* or common presenting feature, as other opportunistic infections and non-specific symptoms are far more frequent.
*Cryptococcal diarrhoea is common*
- **Cryptococcal infection** primarily manifests as **meningitis** or disseminated disease, particularly in adults with advanced HIV.
- While gastrointestinal symptoms can occur, **Cryptococcal diarrhea** is not a common or characteristic presentation of HIV in children.
*Recurrent candidiasis*
- While **recurrent oral candidiasis** (thrush) is common in HIV-infected children, it is often one of the **earliest indicators** and can be present even in less advanced disease.
- However, **recurrent chest infections** generally represent a more significant and debilitating manifestation of immune compromise in pediatric HIV.
Cryptococcosis Indian Medical PG Question 3: A biopsy of a lung nodule from a patient with a history of bird exposure reveals yeast cells with thick capsules. What is the most likely pathogen?
- A. Aspergillus fumigatus
- B. Blastomyces dermatitidis
- C. Histoplasma capsulatum
- D. Cryptococcus neoformans (Correct Answer)
Cryptococcosis Explanation: ***Cryptococcus neoformans***
- The presence of **yeast cells with thick capsules** is a classic histological finding for *Cryptococcus neoformans*.
- While *Cryptococcus* commonly affects immunocompromised individuals, it can also be found in **bird droppings**, particularly from pigeons, making the history of bird exposure relevant.
*Aspergillus fumigatus*
- *Aspergillus fumigatus* typically presents as **hyphae**, not yeast cells, and would not have a thick capsule.
- Infections often manifest as **aspergillomas** (fungus balls) in lung cavities or invasive disease in immunocompromised patients.
*Blastomyces dermatitidis*
- *Blastomyces dermatitidis* appears as **large, broad-based budding yeast cells** but does not possess a thick capsule.
- It is typically found in the **soil**, especially in moist areas, and its association with bird exposure is not as strong as with *Cryptococcus*.
*Histoplasma capsulatum*
- *Histoplasma capsulatum* is characterized by **small intracellular yeast forms** within macrophages and does not have a thick capsule.
- It is strongly associated with **bird and bat droppings** but its microscopic appearance is distinct from that described.
Cryptococcosis Indian Medical PG Question 4: Which of the following is the most common yeast pathogen?
- A. Candida (Correct Answer)
- B. Mucor
- C. Rhizopus
- D. Cryptococcus
Cryptococcosis Explanation: ***Candida***
- **Candida** species, particularly *Candida albicans*, are the **most common cause of fungal infections** worldwide, ranging from superficial mucocutaneous infections to invasive systemic candidiasis.
- They are part of the normal human microbiota and opportunistic pathogens, thriving in conditions like **immunocompromise**, antibiotic use, or presence of medical devices.
*Mucor*
- **Mucor** is a genus of mold, not yeast, and is known to cause **mucormycosis**, a severe and rapidly progressive fungal infection.
- While dangerous, mucormycosis is **much rarer** compared to candidiasis.
*Rhizopus*
- **Rhizopus** is also a genus of mold, not yeast, and is another causative agent of **mucormycosis**, particularly in immunocompromised individuals.
- Like Mucor, infections caused by Rhizopus are **less common** than those caused by Candida.
*Cryptococcus*
- **Cryptococcus neoformans** is a significant yeast pathogen, primarily causing **cryptococcosis**, which often manifests as meningoencephalitis in immunocompromised patients.
- Although it is an important pathogen, its overall incidence is **lower than that of Candida** species.
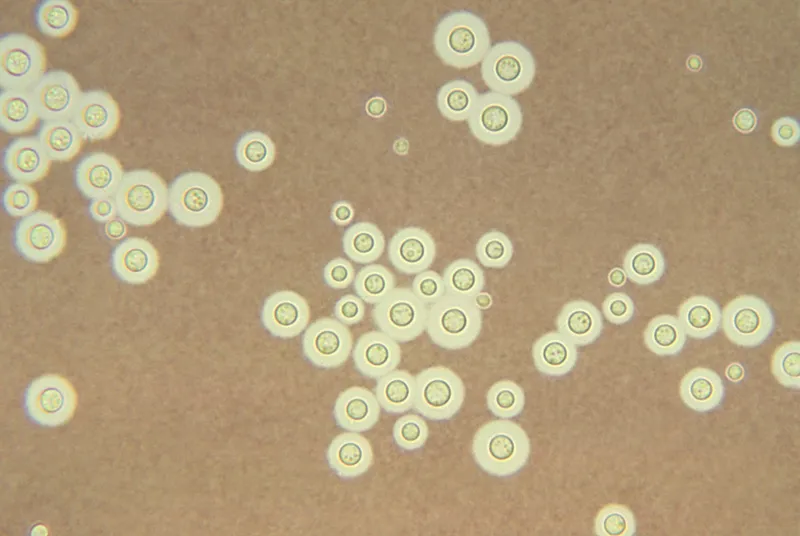
Cryptococcosis Indian Medical PG Question 5: All are correct about the image shown except:
- A. Cryptococcus neoformans
- B. Primary site of infection is CNS (Correct Answer)
- C. Thick polysaccharide capsule
- D. Mucicarmine stain can be used
Cryptococcosis Explanation: ***Primary site of infection is CNS***
- While *Cryptococcus neoformans* is well-known for causing **meningitis** (a CNS infection), the **primary site of infection** is typically the **lungs**, acquired through inhalation of spores. Dissemination to the CNS occurs subsequently, especially in immunocompromised individuals.
*Cryptococcus neoformans*
- The image, showing encapsulated yeast cells with varying sizes and budding, is characteristic of **Cryptococcus neoformans** under India ink stain, where the capsule excludes the ink, creating a halo effect.
- This fungus is known for its distinctive **thick polysaccharide capsule** and its tendency to be found in environments contaminated with bird droppings.
*Thick polysaccharide capsule*
- The clear halo around the yeast cells in the image directly demonstrates the presence of a **thick polysaccharide capsule**, which is a key virulence factor distinguishing *Cryptococcus neoformans*.
- This capsule is responsible for the organism's unique appearance in **India ink preparations** and plays a crucial role in immune evasion.
*Mucicarmine stain can be used*
- The **mucicarmine stain** specifically stains the **polysaccharide capsule** of *Cryptococcus neoformans* bright red, aiding in its identification in tissue samples.
- This stain is a valuable diagnostic tool, particularly when dealing with tissue biopsies where the capsule might not be as distinctly visible with India ink due to cellular debris.
Cryptococcosis Indian Medical PG Question 6: Brain abscess in immunodeficient person is due to :
- A. Aspergillus
- B. Toxoplasma gondii (Correct Answer)
- C. Cryptococcus
- D. Candida
Cryptococcosis Explanation: ***Toxoplasma gondii***
- **Toxoplasma gondii** is a very common cause of **brain abscesses** (cerebral toxoplasmosis) in individuals with compromised immune systems, especially those with AIDS.
- The parasite is usually latent in many people and reactivates when the immune system weakens.
*Aspergillus*
- While *Aspergillus* can cause central nervous system infections, including brain abscesses, this is usually seen in severely **neutropenic** or transplant patients.
- *Aspergillus* typically invades via **hematogenous spread** from a primary pulmonary infection or directly from sinusitis.
*Cryptococcus*
- *Cryptococcus neoformans* is a significant cause of **meningitis** in immunocompromised patients, particularly those with HIV/AIDS.
- While it can cause **cryptococcomas** (focal lesions), pure abscess formation is less common than with *Toxoplasma*.
*Candida*
- *Candida* species can cause **brain microabscesses** or multifocal lesions, especially in patients with disseminated candidiasis originating from prolonged hospitalization or indwelling catheters.
- However, large, solitary brain abscesses are less typical for *Candida* compared to *Toxoplasma gondii*.
Cryptococcosis Indian Medical PG Question 7: After 5 days of birth, a baby developed poor feeding, convulsions, fever, high protein, low sugar, and low chloride levels in the cerebrospinal fluid. This is most likely due to what?
- A. Listeria monocytogenes infection (Correct Answer)
- B. Tuberculosis infection
- C. Leptospira infection
- D. Mycoplasma pneumoniae infection
Cryptococcosis Explanation: ***Listeria monocytogenes infection***
- **Listeria meningitis** in neonates often presents with non-specific symptoms such as **poor feeding**, **convulsions**, and fever, typically in the **first week of life**.
- The CSF profile of **high protein**, **low glucose**, and **low chloride** is characteristic of **bacterial meningitis**, which *Listeria* commonly causes in newborns.
- *Listeria* is one of the leading causes of neonatal meningitis, particularly in early-onset sepsis (within 7 days of birth).
*Tuberculosis infection*
- **Tuberculous meningitis** typically has a more insidious onset and is less common in neonates unless there's significant maternal exposure.
- While it can cause low glucose and high protein in CSF, the acute presentation in a 5-day-old neonate is atypical for TB.
- TB meningitis has a longer incubation period and wouldn't typically present this early.
*Leptospira infection*
- **Leptospirosis** is rare in neonates and usually presents with symptoms like fever, headache, and muscle pain, sometimes leading to renal or hepatic involvement.
- The CSF profile in leptospirosis would typically show **lymphocytic pleocytosis** with normal or slightly elevated protein, not the classic bacterial meningitis pattern.
*Mycoplasma pneumoniae infection*
- **Mycoplasma pneumoniae** is primarily a cause of **respiratory infections** (e.g., atypical pneumonia) in older children and adults.
- It rarely causes meningitis in neonates, and neonatal infection is highly unusual.
- When CNS involvement occurs, it's typically in older children with preceding respiratory symptoms.
Cryptococcosis Indian Medical PG Question 8: Which statement is false regarding Cryptococcus neoformans?
- A. Grows at 5°C and 37°C
- B. Has 4 serotypes
- C. Urease negative (Correct Answer)
- D. Causes superficial skin infection
Cryptococcosis Explanation: **Explanation:**
*Cryptococcus neoformans* is an encapsulated yeast primarily associated with pigeon droppings and is a significant opportunistic pathogen in immunocompromised patients (e.g., HIV/AIDS).
**1. Why "Urease negative" is the False Statement:**
*Cryptococcus neoformans* is characteristically **Urease positive**. The production of the urease enzyme is a key biochemical marker used in the laboratory to differentiate it from other yeasts like *Candida albicans* (which is urease negative). It hydrolyzes urea to produce ammonia, raising the pH and changing the indicator color.
**2. Analysis of Other Options:**
* **Option A (Grows at 5°C and 37°C):** This is true. Unlike many other pathogenic fungi, *C. neoformans* can grow at 37°C (essential for human pathogenicity) and also at lower temperatures like 4°C–5°C.
* **Option B (Has 4 serotypes):** This is true. Based on capsular polysaccharide antigens, it is classified into four serotypes: **A, B, C, and D**. (Note: Serotype A is *C. neoformans var. grubii*, while B and C are now often classified as *C. gattii*).
* **Option D (Causes superficial skin infection):** This is true. While meningitis is the most common presentation, primary or secondary cutaneous cryptococcosis can occur, presenting as papules, pustules, or ulcerations.
**High-Yield Clinical Pearls for NEET-PG:**
* **Virulence Factor:** The **Polysaccharide capsule** (Glucuronoxylomannan) is the most important; it inhibits phagocytosis.
* **Staining:** **India Ink** preparation shows a "halo" (negative staining). **Mucicarmine** stains the capsule red.
* **Culture:** Grows on **Bird Seed Agar** (Niger Seed Agar) producing brown/black colonies due to **Phenoloxidase** activity (melanin production).
* **Drug of Choice:** Induction with Amphotericin B + Flucytosine, followed by Fluconazole.
Cryptococcosis Indian Medical PG Question 9: Which of the following is a non-culturable fungus?
- A. Rhinosporidium (Correct Answer)
- B. Candida
- C. Sporothrix
- D. Penicillium
Cryptococcosis Explanation: **Explanation:**
The correct answer is **Rhinosporidium seeberi**. This organism is unique in medical mycology because it has **never been successfully cultured** on artificial laboratory media (like SDA) or in cell culture. Its classification was historically debated, but molecular analysis (18S rRNA sequencing) has placed it among the *Mesomycetozoea*, a group of aquatic fish parasites, though it is still traditionally studied in Mycology.
**Why the other options are incorrect:**
* **Candida:** A common yeast that grows readily on Sabouraud Dextrose Agar (SDA) within 24–48 hours, forming creamy white colonies.
* **Sporothrix:** A dimorphic fungus that can be cultured at 25°C (mold form with "flower-like" sporulation) and 37°C (yeast form).
* **Penicillium:** A common saprophytic mold that grows rapidly in culture, characterized by its "brush-like" conidiophores.
**High-Yield Clinical Pearls for NEET-PG:**
* **Disease:** Rhinosporidiosis typically presents as **friable, leafy, strawberry-like polypoid masses** in the nose or nasopharynx.
* **Transmission:** Associated with bathing in stagnant freshwater (ponds/tanks).
* **Diagnosis:** Since it cannot be cultured, diagnosis relies on **histopathology**. Look for large **sporangia** (up to 350 µm) containing thousands of **endospores**.
* **Treatment:** Surgical excision with wide-base cauterization is the treatment of choice; medical therapy (Dapsone) has limited efficacy.
Cryptococcosis Indian Medical PG Question 10: Which of the following is not a fungal infection?
- A. Blastomycosis
- B. Cryptococcus
- C. Actinomycosis (Correct Answer)
- D. Histoplasmosis
Cryptococcosis Explanation: **Explanation:**
The correct answer is **Actinomycosis**. Despite its name ending in "-mycosis" (a suffix typically denoting fungal infections), Actinomycosis is caused by **Actinomyces species**, which are **Gram-positive, anaerobic, non-acid-fast bacteria**. They are characterized by filamentous branching growth, which historically led to their misclassification as fungi. However, they lack a chitinous cell wall, possess a prokaryotic nucleus, and are susceptible to antibacterial agents (like Penicillin) rather than antifungals.
**Analysis of Options:**
* **Blastomycosis (A):** A systemic infection caused by the dimorphic fungus *Blastomyces dermatitidis*. It typically presents with pulmonary symptoms or verrucous skin lesions.
* **Cryptococcus (B):** An infection caused by the encapsulated yeast *Cryptococcus neoformans*. It is a major cause of opportunistic meningitis in HIV/AIDS patients.
* **Histoplasmosis (C):** A systemic fungal infection caused by *Histoplasma capsulatum*. It is a dimorphic fungus often associated with bird or bat droppings and mimics tuberculosis clinically.
**High-Yield Clinical Pearls for NEET-PG:**
* **Actinomyces israelii** is the most common human pathogen. It is a normal commensal of the oral cavity and female genital tract.
* **Clinical Hallmark:** Presence of **"Sulfur granules"** (yellowish clumps of organisms) in the pus draining from sinus tracts.
* **Classic Presentation:** "Lumpy jaw" (cervicofacial actinomycosis) following dental trauma or poor oral hygiene.
* **Differential Diagnosis:** Do not confuse *Actinomyces* with *Nocardia*. Both are filamentous bacteria, but **Nocardia is aerobic and weakly acid-fast**, whereas Actinomyces is anaerobic and non-acid-fast.
More Cryptococcosis Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.