

Altitude Physiology - The Thin Air Threat
- Primary Insult: Hypobaric hypoxia due to ↓ barometric pressure ($P_B$) at high altitude.
- Pathophysiology: Lower $P_B$ directly reduces the partial pressure of inspired oxygen ($P_iO_2$), leading to alveolar hypoxia, as described by the Alveolar Gas Equation:
- $P_A O_2 = F_i O_2 (P_B - P_{H_2O}) - (P_a CO_2 / R)$

- Immediate Physiological Response:
Loading diagram…
⭐ The primary, immediate ventilatory response to high altitude is driven by hypoxemia stimulating the peripheral chemoreceptors, not by central chemoreceptors or $CO_2$ levels.
Acclimatization - Adapting to the Apex
-
Immediate (Hours-Days):
- Hyperventilation: ↓ PaCO₂ → respiratory alkalosis.
- Renal Compensation: ↑ Bicarbonate diuresis (via carbonic anhydrase) to normalize pH. Acetazolamide can induce this.
- Cardiovascular: ↑ Heart rate & cardiac output.
-
Chronic (Days-Weeks):
- Erythropoiesis: ↑ Erythropoietin (EPO) from kidneys boosts RBC production.
Loading diagram…
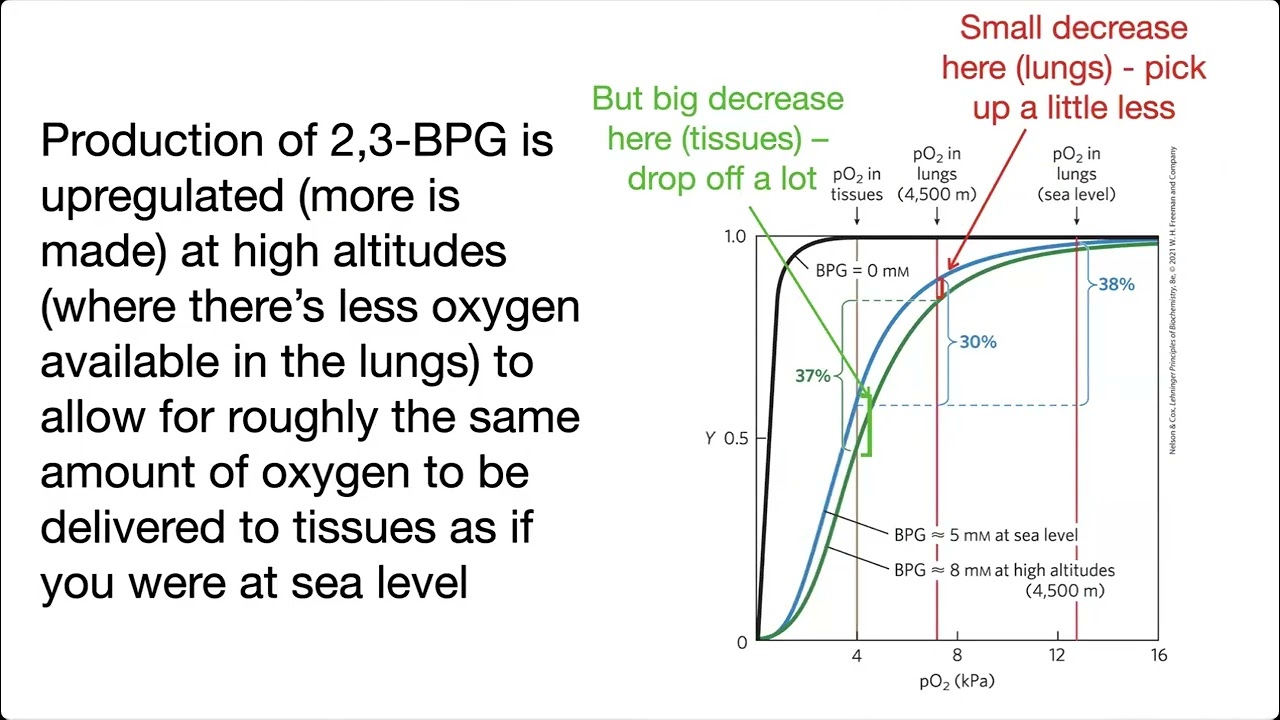
- **Oxygen Unloading:** ↑ **2,3-BPG** shifts oxyhemoglobin curve right, enhancing $O_2$ tissue delivery.
> ⭐ Synthesis of 2,3-BPG in erythrocytes increases with chronic hypoxia, causing a rightward shift of the oxygen-hemoglobin curve, facilitating $O_2$ unloading in tissues.
- **Cellular:** ↑ Angiogenesis (VEGF), ↑ mitochondrial density.
📌 Mnemonic: 'High Altitude Body Compensation': H-A-B-C → Hyperventilation, Acid-base change, BPG (2,3-) increase, Creation of RBCs (EPO).
Mountain Maladies - When Physiology Fails
Failure to acclimatize can lead to life-threatening conditions. Prophylaxis with Acetazolamide 125mg BID can prevent illness.
| Condition | Key Symptoms | Core Pathophysiology | First-line Treatment |
|---|---|---|---|
| AMS | Headache, fatigue, nausea | Mild cerebral edema | Halt ascent, Acetazolamide |
| HACE | Gait ataxia, confusion, worsening AMS | Vasogenic cerebral edema | Descend immediately, Dexamethasone |
| HAPE | Dyspnea at rest, cough (pink, frothy sputum) | Exaggerated hypoxic pulmonary vasoconstriction | Descend immediately, O₂, Nifedipine |
Loading diagram…
High‑Yield Points - ⚡ Biggest Takeaways
- Hypobaric hypoxia is the primary trigger, causing ↓ alveolar (PAO2) and arterial (PaO2) oxygen.
- Hyperventilation is the immediate response, causing respiratory alkalosis, which is later corrected by renal HCO3− excretion.
- Chronic changes include ↑ erythropoietin (EPO) causing polycythemia and ↑ 2,3-BPG shifting the O2-dissociation curve to the right.
- Hypoxic pulmonary vasoconstriction is a key physiologic response that can lead to pulmonary hypertension.
- Acetazolamide prevents/treats Acute Mountain Sickness (AMS) by promoting bicarbonate diuresis.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more