

Microbiology - Stomach's Spiral Squatter

- Gram-negative, spiral-shaped rod colonizing the gastric antrum.
- Highly motile via flagella; catalase, oxidase, and urease-positive.
- Urease neutralizes stomach acid, enabling survival.
- Causes chronic gastritis, peptic ulcers (duodenal > gastric), and is a major risk factor for gastric adenocarcinoma and MALT lymphoma.
- Diagnosis: Urea breath test, stool antigen.
- Treatment: 📌 Triple therapy (Clarithromycin, Amoxicillin, PPI).
⭐ H. pylori is the first formally recognized bacterial carcinogen.
Pathogenesis & Virulence - Acid-Proofing Antics
- Primary Challenge: Survives in the highly acidic (pH 1-2) stomach lumen.
- Key Enzyme: Urease
- Abundantly produced, found on the bacterial surface and cytoplasm.
- Catalyzes urea hydrolysis: $Urea + H_2O \rightarrow 2NH_3 + CO_2$.
- Ammonia ($NH_3$) buffers gastric acid ($HCl$), creating a neutral pH microenvironment.
- This allows the bacterium to burrow into the protective mucus layer.

⭐ CagA (Cytotoxin-associated gene A): An injected oncoprotein delivered by a type IV secretion system. It disrupts the cytoskeleton, increases cell proliferation, and is strongly associated with gastric adenocarcinoma.
Clinical Presentation - Belly's Burning Burden
- Gastritis & Peptic Ulcers: Chronic, gnawing epigastric pain.
- Duodenal Ulcer (>90% assoc.): Pain improves with meals. More common.
- Gastric Ulcer (70% assoc.): Pain worsens with meals.
- Increased Cancer Risk:
- MALT Lymphoma (can regress with H. pylori treatment).
- Gastric Adenocarcinoma.
⭐ The majority of duodenal ulcers are caused by H. pylori, whereas the association is strong but less frequent for gastric ulcers. This is a classic exam distinction.
Diagnosis - Finding the Fiend
-
Non-Invasive Tests (Initial Dx & Eradication Check)
- Urea Breath Test: High sensitivity & specificity. Detects active infection.
- Stool Antigen Assay: Good for initial diagnosis & post-treatment confirmation.
- Serology (IgG): Shows exposure, not active infection; less useful.
-
Invasive Tests (Endoscopy with Biopsy - Gold Standard)
- Rapid Urease Test (RUT): Quick, presumptive ID on biopsy sample.
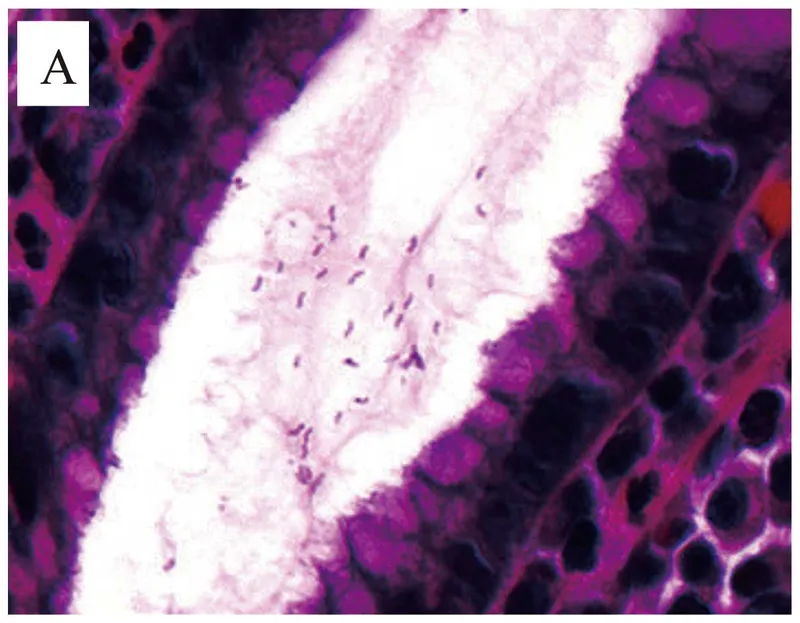
- Histology: Warthin-Starry silver stain reveals spiral-shaped organisms.
- Culture: For antibiotic susceptibility testing, especially in treatment failure.
⭐ The Urea Breath Test relies on H. pylori’s urease splitting labeled urea into ammonia and labeled $CO_2$, which is detected in exhaled breath.
Treatment - Eviction Notice Protocol
- Primary Goal: Eradicate H. pylori to prevent recurrence of peptic ulcers and reduce gastric cancer risk.
- Standard First-Line Therapy (Triple):
- Proton Pump Inhibitor (PPI)
- Clarithromycin
- Amoxicillin (or Metronidazole if penicillin allergic)
- **Quadruple Therapy (First-line in high resistance areas >15% or salvage):
- PPI
- Bismuth subsalicylate
- Metronidazole
- Tetracycline
⭐ For treatment failure, salvage therapy should avoid antibiotics used in the initial regimen. If triple therapy fails, switch to quadruple therapy or a levofloxacin-based regimen.
📌 Mnemonic (Quad Therapy): Please Make Tummy Better (PPI, Metronidazole, Tetracycline, Bismuth).
- H. pylori is a Gram-negative, spiral-shaped bacterium strongly linked to peptic ulcer disease (especially duodenal ulcers), gastric adenocarcinoma, and MALT lymphoma.
- Its key virulence factor is urease, which hydrolyzes urea into ammonia, neutralizing gastric acid and allowing survival in the stomach.
- The urea breath test is a common non-invasive diagnostic method.
- Standard treatment is triple therapy: a proton pump inhibitor (PPI) plus two antibiotics, typically clarithromycin and amoxicillin.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more