

Geriatric Patients - Golden Years, Extra Care
- Physiological Declines:
- CV: ↓ elasticity & CO reserve, ↑ SBP.
- Pulmonary: ↓ FEV1, ↓ VC, ↓ PaO2.
- Renal: ↓ GFR (approx. 1 mL/min/yr post-40), ↓ drug clearance.
- CNS: ↓ brain mass, ↑ BBB permeability, impaired thermoregulation.
- Pharmacology:
- Kinetics: ↑ Vd (lipid-soluble), ↓ Vd (water-soluble), ↓ metabolism & excretion.
- Dynamics: ↑ sensitivity (sedatives, opioids, anticholinergics). "Start low, go slow."
- 📌 Delirium Risk (DELIRIUMS): Drugs, Electrolytes, Lack of drugs, Infection, Reduced senses, Intracranial, Urinary/fecal retention, Myocardial/pulmonary.
⭐ Post-operative delirium is the most common neurological complication in elderly surgical patients, affecting up to 50% in some studies (though the core fact is its commonality).
Pregnant Patients - Two Lives, One Plan
Physiological changes (📌 PREGnancy):
- Cardiac: ↑CO, ↑Plasma Vol. Aortocaval compression >20wks.
- Respiratory: ↓FRC, ↑O₂ consumption.
- GI: ↓LES tone, ↓motility → ↑Aspiration risk.
- Hematologic: Hypercoagulable state.
Anesthesia: Regional preferred. RSI for GA. ↑Difficult airway risk. Surgery Timing: Urgent: anytime. Elective: postpartum. Semi-urgent: 2nd trimester ideal. Avoid 1st & late 3rd.
Key Drugs (Peri-op):
| Safe (Generally) | Avoid/Caution |
|---|---|
| Paracetamol, Opioids | NSAIDs (3rd tri), Warfarin |
| Local Anesthetics, Heparin | ACEi/ARBs, Benzodiazepines |
Loading diagram…
⭐ Left uterine displacement (LUD) by tilting 15-30° left is crucial after 20 weeks gestation to prevent aortocaval compression.
Obese Patients - Weighty Matters, Careful Steps
BMI: $BMI = W (kg) / H (m)^2$. Obesity: BMI ≥ 30 kg/m². Associated Comorbidities: OSA (📌 STOP-BANG), DM, HTN.
Perioperative Risks:
- Airway: Difficult intubation/ventilation (ramped position). ↑Aspiration.
- VTE: ↑DVT/PE. Prophylaxis vital.
- Infection: ↑SSI.
- Pulmonary: Atelectasis, hypoxemia. Respiratory failure.

Anesthetic Challenges:
- Drug Dosing: See table (LBW/IBW/TBW based).
- Positioning: Ramped for airway. Pressure sore risk.
- Ventilation: ↓FRC, ↑airway pressure. PEEP, recruitment.
| Drug | Dosing Weight Basis |
|---|---|
| Propofol (Ind) | LBW / IBW |
| Opioids (Lipo) | IBW / LBW |
| NMBs (Roc, Vec) | IBW / AdjBW |
| NMBs (Sux) | TBW |
| Midazolam | TBW |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | |
| flowchart TD |
Start["📋 STOP-BANG
• Screening tool• OSA Questionnaire"]
Score["⚖️ Score Check
• Result >= 3• Assess risk level"]
HighRisk["⚠️ High OSA Risk
• Perioperative care• CPAP or opioid-safe"]
LowRisk["✅ Low OSA Risk
• Standard care• Routine monitoring"]
Start --> Score Score -->|Yes| HighRisk Score -->|No| LowRisk
style Start fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style Score fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style HighRisk fill:#FDF4F3, stroke:#FCE6E4, stroke-width:1.5px, rx:12, ry:12, color:#B91C1C style LowRisk fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252
> ⭐ Increased risk of post-operative pulmonary complications is a major concern.
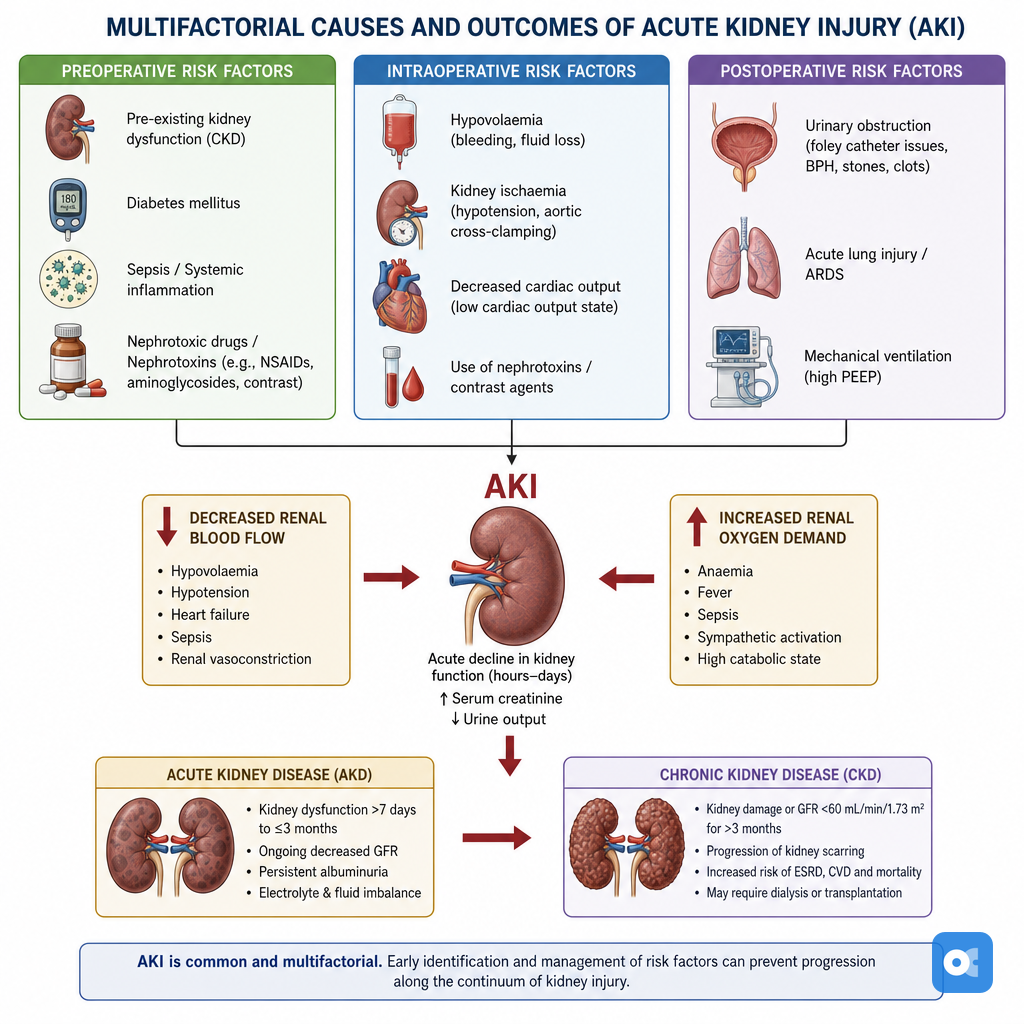
## Renal Dysfunction - Kidney Care, Peri-Op Flair
**CKD Stages (GFR):** G1: ≥**90**; G2: **60-89**; G3a: **45-59**; G3b: **30-44**; G4: **15-29**; G5: <**15**/Dialysis.
**Peri-Op Risks:**
* Fluid/electrolyte issues (K⁺↑, acidosis).
* Drug toxicity (opioids, antibiotics).
* AKI on CKD.
**Key Management:**
* GFR Estimate: Cockcroft-Gault $CrCl = \frac{((140 - Age) \times Wt_{kg})}{(72 \times SCr_{mg/dL})} \times (0.85 \text{ if female})$.
* Adjust doses (see table).
* Dialysis: ≤**24h** pre-op; avoid fistula arm (IV/BP).
* CIN Prevention: IV NS, low/iso-osmolar contrast, avoid NSAIDs.
**Drugs Needing CKD Dose Adjustment:**
| Class | Examples |
|----------------|------------------------------|
| Antibiotics | Penicillins, Ceph, Vanco |
| Anticoagulants | LMWH, Rivaroxaban |
| Analgesics | Opioids (Morphine) |
| Cardiovascular | Digoxin, ACEi/ARBs |> ⭐ Meperidine contraindicated in CKD: normeperidine (neurotoxic) accumulation.
## High‑Yield Points - ⚡ Biggest Takeaways
> * **Elderly**: ↑ risk of **postoperative delirium** & **cardiac events**; manage **polypharmacy**.
> * **Obesity**: ↑ risk of **VTE**, **wound infection**, **OSA**; optimize **respiratory function**.
> * **Pregnancy**: Safest surgery in **2nd trimester**; avoid **NSAIDs** (3rd trimester), minimize **radiation**.
> * **Diabetes**: Target glucose **140-180 mg/dL**; monitor for **DKA/HHS**, ↑ **SSI** risk.
> * **CKD**: **Dose adjust** drugs; avoid **nephrotoxins**; monitor for **AKI**, **electrolyte imbalance**.
> * **Liver Disease**: Assess **coagulopathy** (INR); risk of **bleeding**, **encephalopathy**; use **Child-Pugh**.
> * **HIV**: Continue **ART**; assess **CD4/viral load**; ↑ risk of **opportunistic infections**.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more