

CVI Intro & Pathophysiology - Vein Valve Vexations
- CVI: Syndrome of chronic impaired venous return, primarily from lower limbs, due to venous hypertension.
- Core Problem: Incompetent venous valves ("Vein Valve Vexations").
- Primary CVI (~70-80%): Degenerative valvular reflux; inherent weakness of vein wall/valves.
- Secondary CVI (~20-30%): Post-thrombotic syndrome (PTS) after DVT; or non-thrombotic iliac vein obstruction causing outflow obstruction.
- Pathophysiological Sequence:
- Valve failure → retrograde blood flow (reflux).
- Calf muscle pump dysfunction (failure to ↓ venous pressure during ambulation).
- Sustained venous hypertension → capillary leakage, leukocyte trapping, inflammation, fibrin cuffing.
- Manifests as: edema, skin changes (e.g., lipodermatosclerosis, stasis dermatitis/eczema), and ultimately venous ulcers.
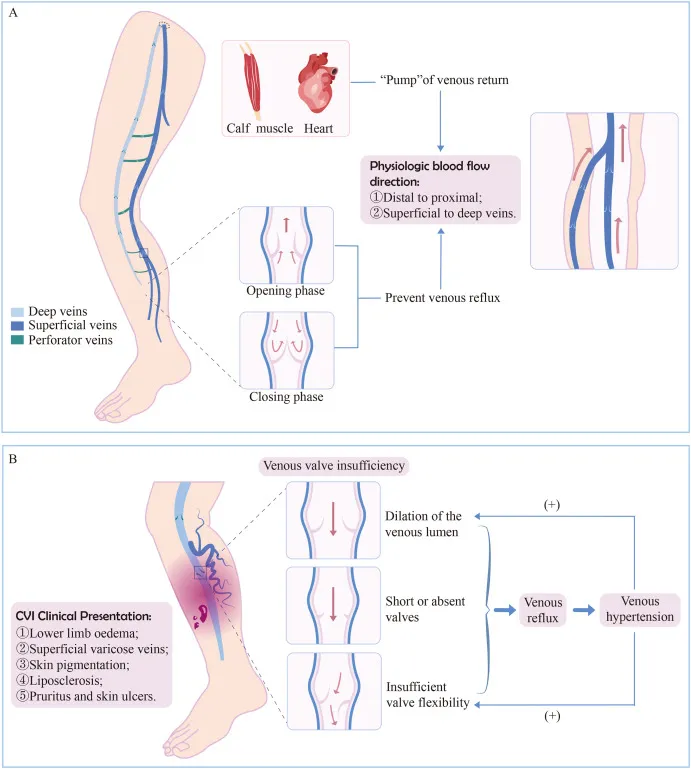
⭐ Calf muscle pump failure is a key contributor to venous hypertension and CVI progression.
CVI Clinical Picture & CEAP - Leggy Load & Looks
- Symptoms (Leggy Load):
- Ache, heaviness, cramps; worse with dependency, better with elevation.
- Leg swelling, pruritus.
- 📌 Mnemonic - ACHES: Aching, Cramps, Heaviness, Edema, Skin changes.
- Signs (Leggy Looks):
- Telangiectasias (<1 mm), reticular veins (1-3 mm), varicose veins (>3 mm).
- Edema (pitting).
- Skin changes:
- Pigmentation (hemosiderin).
- Dermatitis/eczema.
- LDS: induration, 'inverted champagne bottle'.
- Atrophie blanche.
- Venous ulcers (medial malleolus, shallow).
⭐ Corona phlebectatica (fan-shaped intradermal veins at ankle/foot) is an early sign of advanced CVI (CEAP C4).
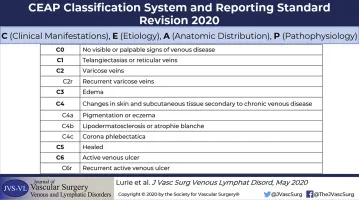
- CEAP Classification:
- Clinical (C0-C6, S/A):
- C0: No signs.
- C1: Telangiectasias/reticular.
- C2: Varicose veins.
- C3: Edema.
- C4a: Pigmentation/eczema.
- C4b: LDS/atrophie blanche.
- C5: Healed ulcer.
- C6: Active ulcer.
- (S/A for symptoms)
- E: Ec (Congenital), Ep (Primary), Es (Secondary).
- A: As (Superficial), Ad (Deep), Ap (Perforator).
- P: Pr (Reflux), Po (Obstruction), Pr,o (Both).
- Clinical (C0-C6, S/A):
CVI Diagnosis & Workup - Vein Viewing Quest
- Clinical Evaluation:
- Symptoms: Leg ache, swelling, heaviness.
- Signs: Edema, varicose veins, skin changes (lipodermatosclerosis, ulceration).
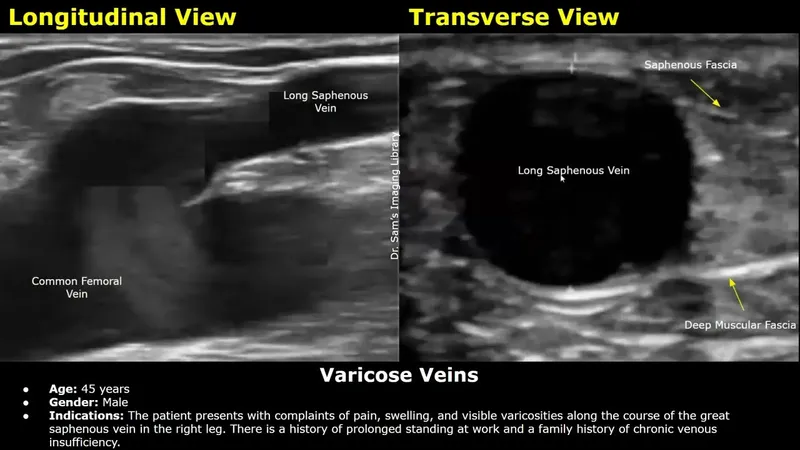
- Duplex Ultrasound (DUS):
- Primary diagnostic tool.
- Identifies reflux & obstruction.
⭐ Duplex ultrasound is the gold standard for diagnosing CVI, identifying reflux >0.5s in superficial/perforator veins or >1s in deep veins.
- Ancillary Tests (selected cases):
- Venography, Plethysmography (APG), Ambulatory Venous Pressure (AVP).
CVI Management Strategies - Flow Fixes & Fortifiers
- Foundation (All CEAP Stages): 📌 Mnemonic: LEGS
- Leg elevation, Exercise (calf pump), Graduated compression, Skin care.
- Compression: Key! Stockings (20-30 mmHg for C0-C2, 30-40 mmHg for C3-C6), multi-layer bandages.
⭐ Compression therapy (e.g., 30‑40 mmHg stockings) is the cornerstone of CVI management, especially for CEAP C3-C6 stages.
- Pharmacotherapy (Adjunctive):
- Venoactive drugs (VADs; e.g., MPFF, diosmin): ↑venous tone, ↓capillary permeability, ↓edema.
- Pentoxifylline: Aids ulcer healing (↑RBC flexibility). Sulodexide also used.
- Interventions (For reflux/symptoms; CEAP C2-C6):
- Endovenous Ablation:
- Thermal: Radiofrequency (RFA), Laser (EVLA) for axial reflux.
- Non-Thermal Non-Tumescent (NTNT): Cyanoacrylate, MOCA.
- Sclerotherapy: Foam/liquid for varicosities, tributaries.
- Surgery: Ligation & stripping (less common), phlebectomy, SEPS (perforators).
- Endovenous Ablation:
- Venous Ulcer Care (CEAP C5-C6):
- Debridement, dressings, sustained high compression, consider pentoxifylline/sulodexide.

High‑Yield Points - ⚡ Biggest Takeaways
- Valvular incompetence and calf muscle pump dysfunction cause venous hypertension.
- Key symptoms include leg aching/heaviness, edema, and skin changes (e.g., lipodermatosclerosis, hemosiderin staining).
- Venous ulcers are classically found near the medial malleolus.
- Duplex ultrasonography is the gold standard for diagnosis.
- Graduated compression therapy and leg elevation are mainstays of conservative treatment.
- The CEAP classification is crucial for staging severity.
- History of DVT is a significant predisposing factor.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more