

Appendicitis: Anatomy & Etiopathogenesis - Gut's Grumpy Nook
- Anatomy Essentials:
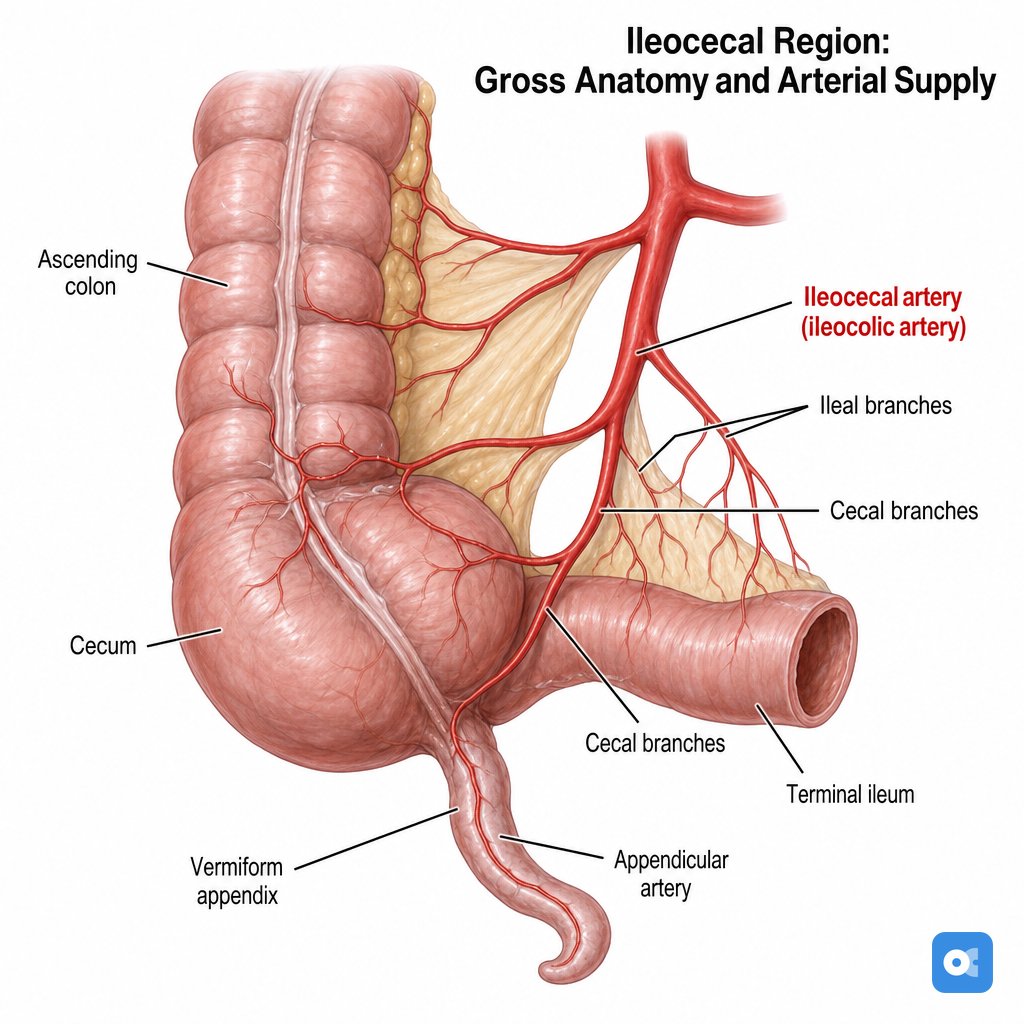
- True diverticulum of caecum; base at confluence of 3 taeniae coli.
- 📌 Mnemonic: "Taeniae meet At The Appendix base."
- Surface marking: McBurney's point (junction of lateral ⅓ & medial ⅔, umbilicus to ASIS line).
- Most common position: Retrocaecal (~65-70%). Others: pelvic, subcaecal, pre/post-ileal.
- Blood supply: Appendicular artery (end-artery from ileocolic artery).
- Innervation: Sympathetic & visceral afferents via T10 (initial periumbilical pain).
- True diverticulum of caecum; base at confluence of 3 taeniae coli.
- Etiopathogenesis:
- Core mechanism: Luminal obstruction.
- Adults: Fecolith (most common).
- Children: Lymphoid hyperplasia (most common).
- Others: Parasites (e.g., Ascaris), carcinoid tumor, foreign body, strictures.
- Pathophysiology Cascade:
- Core mechanism: Luminal obstruction.
Loading diagram…
* 
> ⭐ The lifetime risk of developing appendicitis is approximately **7-8%**.
Appendicitis: Clinical Features - Pain's Pointed March
- Pain Trajectory (Classic):
- Onset: Dull, periumbilical, colicky (visceral).
- Migration (📌 "Pointed March"): To Right Iliac Fossa (RIF) within 12-24 hrs.
- Character: Sharp, constant, localized at McBurney's point.
- Key Associated Symptoms:
- Anorexia: Often first, highly consistent.
- Nausea/Vomiting: Typically after pain onset.
- Fever: Low-grade (< 38.5°C).
- Physical Exam Signs:
- RIF tenderness, guarding, rebound.
- Special Tests: Rovsing's, Psoas, Obturator signs positive.

⭐ The sequence of symptoms is crucial: anorexia, then vague abdominal pain, then vomiting, then localization of pain to RIF and fever development (Dieulafoy's triad for sequence: pain, nausea/vomiting, fever).
Appendicitis: Diagnosis & DDx - Case of the Coded Clues
- Clinical Scoring:
- Alvarado Score (MANTRELS - Migratory RIF pain, Anorexia, Nausea/Vomiting, Tenderness RIF, Rebound, Elevated temp, Leukocytosis, Shift to left): Max 10.
- Score ≤4: Appendicitis unlikely.
- Score 5-6: Equivocal → Image.
- Score ≥7: High probability → Surgery consult.
- Appendicitis Inflammatory Response (AIR) Score: Max 12. Similar interpretation.
- Alvarado Score (MANTRELS - Migratory RIF pain, Anorexia, Nausea/Vomiting, Tenderness RIF, Rebound, Elevated temp, Leukocytosis, Shift to left): Max 10.
- Lab Tests:
- ↑WBC (Neutrophilia, left shift).
- ↑C-Reactive Protein (CRP).
- Imaging:
- Ultrasound (USG): First-line in children & pregnant women. Appendix diameter >6mm, non-compressible, target sign, appendicolith.
- Contrast-Enhanced CT (CECT) Abdomen: Gold standard. Dilated appendix >6mm, wall thickening, peri-appendiceal fat stranding, appendicolith.
⭐ CECT abdomen has a sensitivity and specificity of >95% for acute appendicitis.
- Differential Diagnosis (DDx):
- Gastrointestinal: Mesenteric adenitis, Meckel's diverticulitis, Crohn's disease, diverticulitis.
- Gynecological: Ectopic pregnancy, Pelvic Inflammatory Disease (PID), ovarian torsion/cyst rupture.
- Urological: Ureteric colic, Pyelonephritis/UTI.
- Diagnostic Pathway:
Appendicitis: Management & Complications - Snip, Stitch, Sidestep
- Initial Steps: NPO, IV fluids, analgesia, broad-spectrum IV antibiotics (e.g., Ceftriaxone + Metronidazole).
- Definitive Management:
- Appendectomy: Gold standard.
- Laparoscopic: Preferred; ↓pain, ↓stay, faster recovery.
- Open: McBurney’s or Lanz incision.
- Non-Operative Management (NOM): For selected uncomplicated cases with antibiotics. Recurrence risk ~20-30% within 1 year.
- Appendectomy: Gold standard.
- Specific Scenarios:
- Appendicular Mass: Initial conservative (Ochsner-Sherren regime). Consider interval appendectomy after 6-8 weeks.
- Appendicular Abscess: Percutaneous drainage + antibiotics. If drainage fails/unavailable → surgery. ⭐ > The most common overall complication following appendectomy is wound infection.
Loading diagram…
- Key Complications:
- Perforation (esp. extremes of age)
- Wound Infection (most common)
- Intra-abdominal/Pelvic Abscess
- Stump Appendicitis
- Adhesive Small Bowel Obstruction (late)
- Portal Pyemia (septic pylephlebitis - rare)
High‑Yield Points - ⚡ Biggest Takeaways
- McBurney's point tenderness is the most reliable clinical sign.
- Alvarado score (MANTRELS) aids diagnosis; score ≥7 strongly suggests appendicitis.
- USG is initial imaging (children/pregnant); CT scan is most accurate for adults.
- Perforation is the most common serious complication, leading to peritonitis.
- Standard treatment is appendectomy (laparoscopic preferred).
- Obturator and Psoas signs may indicate a retrocecal appendix.
- Key DDx: mesenteric adenitis, ectopic pregnancy, PID, Meckel's diverticulitis.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more