

Colon Anatomy - The Winding Road

- Segments & Average Lengths:
- Cecum: Pouch with ileocecal valve. Appendix (artery: appendicular a.) arises posteromedially.
- Ascending Colon: ~15 cm. Retroperitoneal.
- Hepatic Flexure
- Transverse Colon: ~50 cm. Intraperitoneal (transverse mesocolon), omental attachment.
- Splenic Flexure
- Descending Colon: ~25 cm. Retroperitoneal.
- Sigmoid Colon: ~40 cm. Intraperitoneal (sigmoid mesocolon), mobile.
⭐ The sigmoid colon is the most common site for volvulus due to its mobility and long mesentery.
- External Features:
- Taeniae Coli: 3 longitudinal muscle bands (mesocolic, omental, free); converge at appendix base.
- Haustra: Sacculations of the colon wall.
- Appendices Epiploicae: Fat-filled peritoneal tags.
- Peritoneal Relations:
- Intraperitoneal: Cecum (variable), Transverse Colon, Sigmoid Colon.
- Retroperitoneal: Ascending Colon, Descending Colon. (📌 Partial SAD PUCKER: C for Colon parts).
Rectoanal Anatomy - The Final Stretch
- Rectum: ~12-15 cm; Sacral & Anorectal flexures (puborectalis); Ampulla; 3 Valves of Houston.
- Anal Canal: Anatomical ~3.8-4 cm, Surgical ~4 cm.
- Dentate Line: ~2 cm from anal verge; hindgut/proctodeum junction.
Feature Above Below Epithelium Columnar Stratified Squamous Blood (Art/Ven) Sup. Rectal A./V. (Portal) Inf. Rectal A./V. (Caval) Lymph Internal Iliac nodes Superficial Inguinal nodes Nerves Autonomic (insensitive) Somatic (Pudendal N. - sensitive) Hemorrhoids Internal (painless) External (painful) - Columns of Morgagni, anal crypts/glands (infection → fistula-in-ano). Hilton's line (intersphincteric groove).
- Dentate Line: ~2 cm from anal verge; hindgut/proctodeum junction.
- Sphincters:
- Internal (IAS): Smooth muscle, involuntary (Sympathetic tone ↑, Parasympathetic relax ↓).
- External (EAS): Striated muscle, voluntary (Pudendal N.), 3 parts.
- Anorectal Ring: Puborectalis, IAS, EAS; crucial for continence.
⭐ The dentate line is a key landmark differentiating internal and external hemorrhoids.
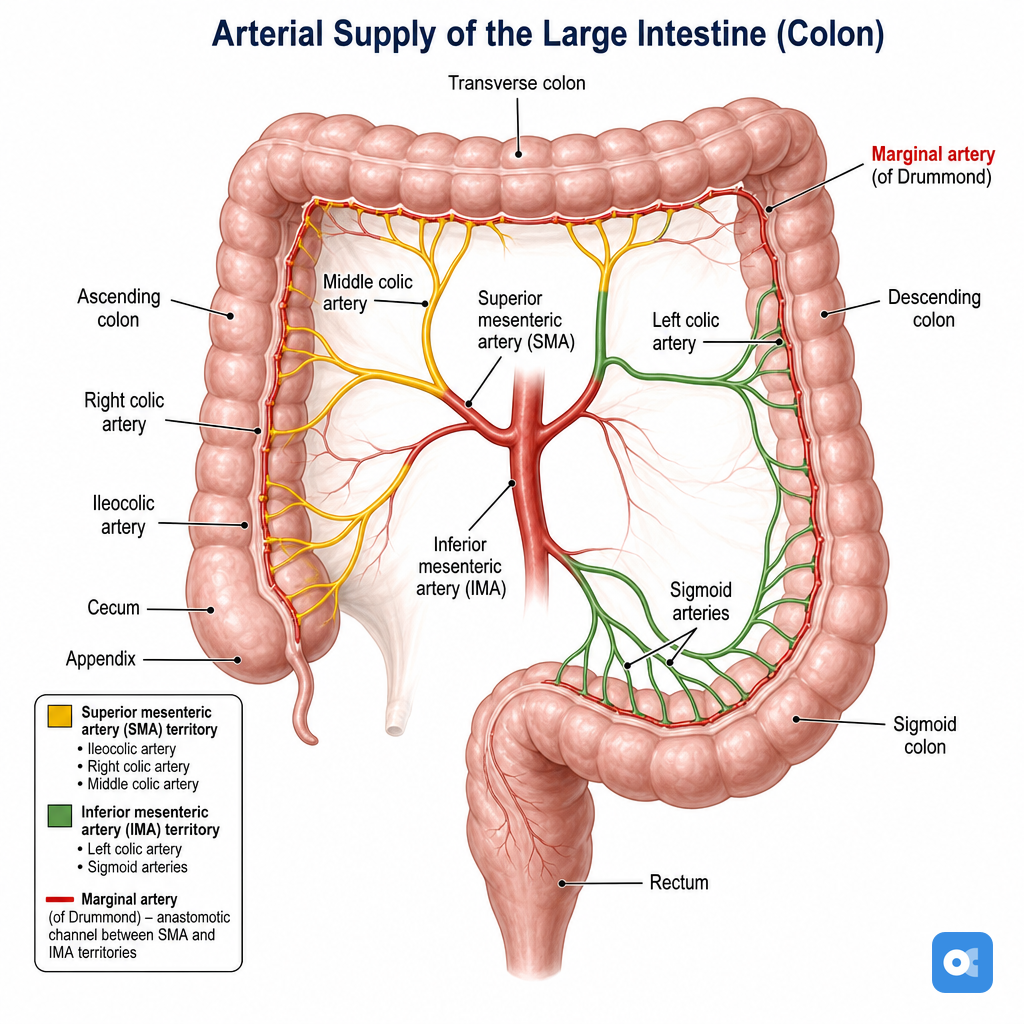
Vascular & Neural - Pipes & Wires
- Arterial Supply:
- SMA branches: Ileocolic, Right Colic, Middle Colic.
- IMA branches: Left Colic, Sigmoid Arteries, Superior Rectal Artery (📌 LSS).
- Anastomoses: Marginal artery of Drummond, Arc of Riolan (variable).
- Critical Points: Griffiths' point (splenic flexure), Sudeck's point (rectosigmoid junction).
Loading diagram…
- Venous Drainage: Parallels arteries.
- SMV, IMV (drains to splenic vein).
- Superior rectal vein (portal); Middle & Inferior rectal veins (systemic; portocaval anastomosis).
- Lymphatic Drainage: Follows arterial supply (epicolic, paracolic, intermediate, principal nodes).
- Above dentate line: to internal iliac nodes.
- Below dentate line: to superficial inguinal nodes.
- Innervation:
- Sympathetic: T10-L2 (via splanchnic nerves, hypogastric plexuses) → ↓motility, contracts IAS.
- Parasympathetic: Vagus (proximal to splenic flexure); Pelvic splanchnics (S2-S4) (distal colon, rectum) → ↑motility, relaxes IAS.
- Somatic: Pudendal nerve (S2-S4) → EAS, perineal sensation.
⭐ Sudeck's critical point is located at the origin of the last sigmoid artery from the IMA; ligation proximal to it may compromise rectal blood supply.
Micro & Function - Guts at Work
- Histology (Layers): Mucosa, Submucosa (Meissner's plexus), Muscularis Externa, Serosa/Adventitia.
- Colon Mucosa: Simple columnar, ↑goblet cells, absorptive cells. Crypts of Lieberkühn, no villi.
- Muscularis Externa: Inner circular, outer longitudinal (3 taeniae coli). Auerbach's (intermuscular) plexus.
- Anal Canal: Epithelial transition (dentate line): Columnar → Strat. Sq. Non-Ker. → Strat. Sq. Ker. (below Hilton's line).
- Physiology:
-
Absorption: Water (1-1.5L/day), electrolytes (Na+, Cl-), SCFAs (butyrate).
⭐ Butyrate, a short-chain fatty acid, is the preferred energy source for colonocytes.
-
Secretion: Mucus (lubrication).
-
Motility: Haustra (mixing), Mass movements (propulsion, 1-3/day). Gastro/Duodenocolic reflexes.
-
Defecation: Rectal distension initiates reflex.
-
Microbiota: Vit K & B synthesis, fermentation, immune modulation.
-
High‑Yield Points - ⚡ Biggest Takeaways
- Rectal arteries: Superior (from IMA), Middle (from Internal Iliac), Inferior (from Internal Pudendal).
- Dentate line: Divides columnar epithelium (endoderm, visceral afferents) above from squamous epithelium (ectoderm, somatic afferents) below.
- Rectal lymphatics: Upper/middle rectum drains to pararectal & IMA nodes; lower rectum to internal iliac nodes.
- Anal canal lymphatics: Above dentate line to internal iliac nodes; below dentate line to superficial inguinal nodes.
- Anal sphincters: Internal anal sphincter (involuntary, sympathetic tone); External anal sphincter (voluntary, pudendal nerve S2-S4).
- Valves of Houston: Usually three transverse rectal folds; the middle is largest and most constant, around 11 cm from anal verge.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more