

DWI Basics - Water Wobbles Tell Tales
- Brownian Motion: Constant, random thermal motion of water molecules.
- In tissues, this "wobble" is hindered by cell membranes, organelles, and macromolecules, reflecting tissue microstructure.
- b-value: Key DWI parameter controlling diffusion weighting.
- Determined by gradient pulse strength, duration, and interval.
- Higher b-value (e.g., 1000 s/mm²) → ↑ sensitivity to restricted diffusion, ↓ signal from freely diffusing water.
- ADC (Apparent Diffusion Coefficient): Quantifies this water mobility (detailed next).

⭐ DWI is highly sensitive for acute ischemic stroke, often positive within minutes of onset.
ADC Interpretation - Decoding Diffusion's Dance
- Apparent Diffusion Coefficient (ADC) map: Quantifies water molecule mobility, derived from DWI.
- Low ADC (Dark on map): True restricted diffusion.
- Cytotoxic edema (e.g., acute stroke, cellular tumors).
- High ADC (Bright on map): Facilitated diffusion.
- Vasogenic edema, cysts, chronic infarcts.
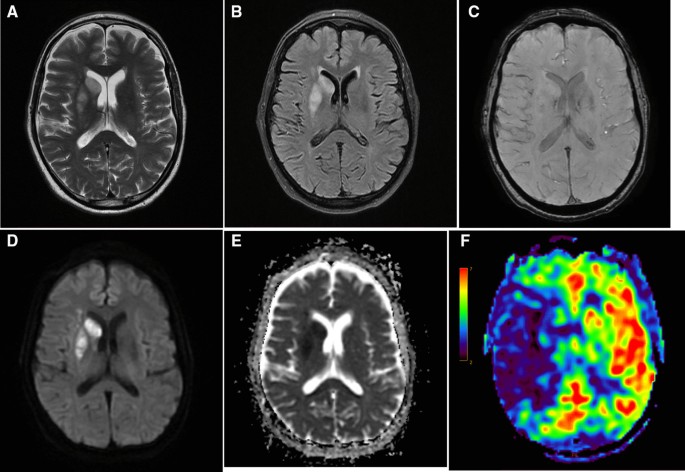
- T2 Shine-through vs. True Restriction:
- True Restriction: DWI ↑, ADC ↓ (e.g., acute stroke).
- T2 Shine-through: DWI ↑, ADC ↑ (lesion bright on T2, no true restriction).
Loading diagram…
⭐ In acute stroke, DWI shows high signal and ADC shows low signal due to restricted water diffusion in cytotoxic edema.
DTI & Tractography - Neural Highways Exposed
- Diffusion Tensor Imaging (DTI): Measures directionality of water diffusion in tissues, especially white matter.
- Diffusion Tensor: Describes magnitude & direction of water diffusion in 3D.
- Fractional Anisotropy (FA): Degree of directional preference (0=isotropic, 1=anisotropic).
- Mean Diffusivity (MD): Average diffusion rate.
- FA Color Maps: Visualize tract orientation:
- Red: Left-Right (e.g., corpus callosum)
- Blue: Superior-Inferior (e.g., corticospinal tracts)
- Green: Anterior-Posterior (e.g., cingulum)
- Tractography: 3D reconstruction of white matter tracts. Applications: pre-surgical planning, assessing white matter injury (e.g., TBI, stroke), neurodegenerative diseases.
⭐ DTI is used to assess white matter tract integrity and directionality, crucial in conditions like traumatic brain injury or for surgical planning near eloquent pathways.
Perfusion Techniques - Blood Flow Blueprint
Assesses blood delivery to tissues, crucial for evaluating tissue viability.
- Dynamic Susceptibility Contrast (DSC-MRI):
- Principle: Bolus tracking of T2* contrast agent (e.g., Gadolinium) causing signal drop.
- Parameters: Cerebral Blood Volume (CBV), Cerebral Blood Flow (CBF), Mean Transit Time (MTT), Time To Peak (TTP).
- Formula: $CBF = CBV / MTT$.
- Dynamic Contrast-Enhanced (DCE-MRI):
- Principle: T1 contrast agent leakage into extravascular extracellular space (EES).
- Parameters: $K^{trans}$ (volume transfer constant), $V_e$ (EES volume fraction), $V_p$ (plasma volume fraction).
- Arterial Spin Labeling (ASL):
- Non-contrast technique; magnetically labels arterial blood water as an endogenous tracer.
⭐ Cerebral Blood Volume (CBV) derived from perfusion imaging is often ↑ in high-grade gliomas and can help differentiate tumor recurrence from radiation necrosis (which typically shows ↓ CBV).
Clinical Perfusion - Stroke & Tumor Power
- Acute Stroke:
- Core (DWI lesion) vs. Penumbra (PWI/DWI mismatch = salvageable tissue).
- Guides reperfusion therapy decisions.
Loading diagram…
- Brain Tumors:
- Grading: ↑ Cerebral Blood Volume (CBV) suggests high-grade glioma.
- Distinguishes tumor (high CBV) from non-neoplastic lesions (e.g., abscess, tumefactive MS often show lower CBV).
- Monitors treatment response (e.g., ↓CBV post anti-angiogenic therapy).
- Other Uses: Differentiates pseudo-progression (treatment effect) from true tumor progression.
⭐ The DWI/PWI mismatch concept is critical for identifying the ischemic penumbra, representing salvageable tissue in acute stroke patients eligible for reperfusion therapies.
High‑Yield Points - ⚡ Biggest Takeaways
- DWI is crucial for early acute ischemic stroke detection (hyperintense).
- ADC maps confirm true restriction (hypointense) in acute ischemia.
- Perfusion imaging (CBF, CBV, MTT) assesses tissue viability and penumbra.
- DWI-PWI mismatch indicates salvageable brain tissue (ischemic penumbra).
- Restricted diffusion (low ADC): also in abscesses, cellular tumors, CJD.
- Beware T2 shine-through: DWI bright but ADC not low.
- In tumors, ↑CBV on perfusion often suggests high-grade malignancy.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more