

Initial Assessment - 🚦 Spine Alert Rules
Decision tools for selective C-spine imaging, minimizing radiation.
- NEXUS (National Emergency X-Radiography Utilization Study) Criteria: Clears C-spine if all 5 criteria negative:
- No posterior midline cervical tenderness
- No intoxication
- Alertness normal (GCS 15)
- No focal neurological deficit
- No painful distracting injury
- Canadian C-Spine Rule (CCR): For alert (GCS 15), stable trauma patients. More complex but higher accuracy.
Loading diagram…
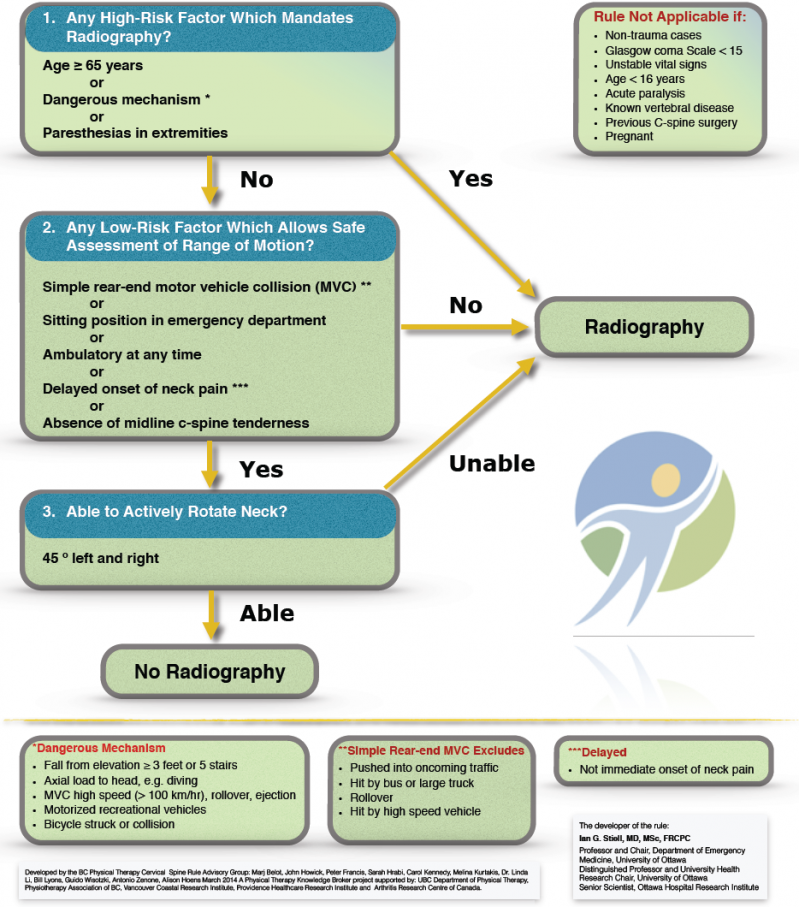
⭐ CCR demonstrates higher sensitivity and specificity than NEXUS for clinically significant C-spine injuries.
Imaging Modalities - 📸 Pixel Power Play
- X-ray (Plain Radiographs):
- Initial screening in low-risk patients (e.g., fulfilling NEXUS criteria for C-spine clearance if imaging still pursued) or resource-limited settings.
- Standard views: AP, lateral; odontoid for C-spine.
- Assesses alignment, gross fractures. Limited for subtle injuries & soft tissues.
- CT (Computed Tomography):
- Primary modality for suspected spine trauma, especially unstable injuries.
- Superior for bony detail, complex fractures, pre-operative planning.
- Multiplanar Reconstructions (MPR) essential.
⭐ CT is the investigation of choice for definitive evaluation of osseous spinal trauma.
- MRI (Magnetic Resonance Imaging):
- Best for neurological deficits, suspected spinal cord injury (SCI), ligamentous injury, epidural hematoma.
- Use if CT negative but symptoms persist or to assess soft tissue extent.
Cervical Spine Injuries - 💔 Neck Wrecks
- C1 (Atlas):
- Jefferson Fracture: Burst # of C1 ring. Rule of Spence: Lateral mass displacement >7mm on open-mouth X-ray suggests transverse ligament injury.
- C2 (Axis):
- Odontoid (Dens) Fractures:
- Type I: Tip avulsion (stable).
- Type II: Base of dens (unstable, common).
- Type III: Extends into C2 body (unstable, good prognosis).
- Hangman's Fracture: Bilateral C2 pars/pedicle # from hyperextension (unstable).
- Odontoid (Dens) Fractures:
- Lower Cervical (C3-C7) Injuries:
- Flexion Teardrop Fracture: Anteroinferior vertebral body fragment; highly unstable (ligamentous disruption).
- Clay-Shoveler's Fracture: Spinous process avulsion (C7>C6); stable.
- Stability Assessment:
- Denis 3-column theory; ≥2 columns disrupted = unstable.

⭐ Type II Odontoid fracture is the most common type and carries a high risk of non-union, making it unstable.
Thoracolumbar Trauma - 💥 Back Breakers
- Denis Columns: Stability: 3-column model.
- Anterior, Middle, Posterior.
- ≥2 columns failed = Unstable.
- Key Fracture Types:
- Compression: Anterior column fails (wedge). Often stable.
- Burst: Anterior + Middle fail; retropulsion common; neuro risk.
- Chance: Flexion-distraction (📌 seatbelt); horizontal #, 3 columns; PLC often disrupted.
- Fracture-Dislocation: Grossly unstable; 3 columns disrupted, displaced.
- Imaging: X-ray (initial); CT (bone detail); MRI (cord/ligaments/PLC).
- TLICS Score: Guides management (Morphology, Neuro, PLC).
- Score >4 → surgery.
Loading diagram…
⭐ TLICS: PLC disruption scores 3 points, strongly favoring surgery due to critical instability.
Special Considerations - 🤔 Tricky Spines
- Pediatric Spine: SCIWORA (Spinal Cord Injury Without Radiographic Abnormality) - MRI crucial. Pseudosubluxation (C2-C3 common).
- Osteoporotic Fractures: Insufficiency fractures; may be occult on X-ray. Consider CT/MRI.
- Ankylosing Spondylitis: ↑Risk of unstable "chalkstick" fractures even with minor trauma.
- Cord Syndromes: Clinical patterns (Central, Brown-Séquard, Anterior, Posterior) guide diagnosis.
⭐ Central Cord Syndrome: Most common incomplete lesion; upper limbs affected more than lower; often in elderly with hyperextension injury.
- Degenerative Spine: Pre-existing changes can complicate assessment; differentiate acute vs. chronic findings.
High‑Yield Points - ⚡ Biggest Takeaways
- CT is gold standard for suspected cervical spine trauma.
- MRI is superior for ligamentous injuries, spinal cord assessment, and epidural hematoma.
- NEXUS criteria and Canadian C-Spine Rule guide imaging in alert, stable trauma patients.
- Odontoid fractures: Type II is most common and unstable.
- Recognize unstable patterns: Jefferson fracture (C1 burst), Hangman's fracture (C2 bilateral pedicles).
- Chance fracture indicates a flexion-distraction mechanism, often with seatbelt use.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more