

DBT Fundamentals - Slicing Through Density
- Digital Breast Tomosynthesis (DBT): A quasi-3D X-ray imaging technique.
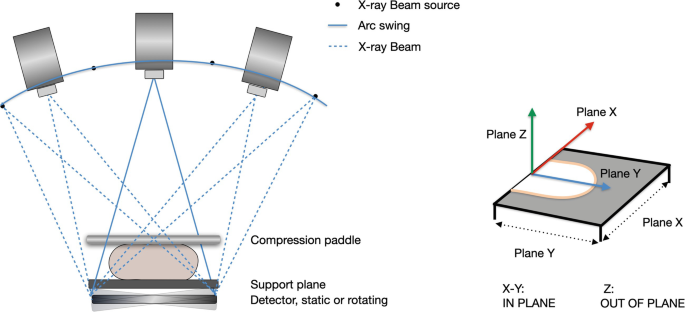
- Acquires multiple low-dose projection images over a limited arc across the breast.
- Reconstructs images into thin slices (typically 1 mm), like a CT scan.
- Primary Advantage: Reduces tissue superposition, a major limitation of 2D mammography.
- Improves lesion visibility, especially in dense breasts.
- Better characterization of masses, architectural distortions, and asymmetries.
- Clinical Impact:
- ↑ Cancer Detection Rate (CDR).
- ↓ Recall rates (fewer false positives).

⭐ DBT improves invasive cancer detection rates by approximately 1-2 additional cancers per 1000 women screened and reduces recall rates by 15-30% compared to 2D mammography alone.
DBT Technique & Workflow - The Tomo Tango
- Acquisition Principle: X-ray tube moves in an arc (e.g., 15-50°) around the compressed breast.
- Acquires multiple low-dose projection images (typically 9-25).
- Total radiation dose often comparable to, or slightly higher than, 2D mammography.
- Image Reconstruction:
- Algorithms (e.g., Filtered Back Projection, Iterative Reconstruction) process projection data.
- Generates a series of thin (e.g., 1 mm) high-resolution slices.
- Allows "scrolling" through breast tissue, minimizing superimposition.
- Clinical Workflow:
Loading diagram…
> ⭐ DBT significantly improves cancer detection rates and reduces recall rates, particularly in women with dense breast tissue, by minimizing the effect of overlapping fibroglandular tissue.
DBT in Action - Spotting the Culprit
- Dense Breasts:
- ↓ Tissue overlap, ↑ lesion visibility.
- ↑ Cancer detection (esp. invasive).
- ↓ False positives & recall rates (15-40%).
- Asymmetries:
- Precise 3D localization (focal, global, developing).
- Distinguishes true lesions vs. summation artifacts.
- Architectural Distortions (AD):
- ↑ Detection of subtle AD (spiculations, retractions).
- Better AD characterization & extent.
- BI-RADS Assessment:
- ↑ Diagnostic accuracy; aids BI-RADS re-classification (e.g., 0→1/2; 3→4).
- ↑ Confidence for BI-RADS 1 & 2.
- Problem-solving for BI-RADS 0, 3, 4.
⭐ DBT has shown a significant reduction in recall rates (up to 40%) and an increase in invasive cancer detection rates (by 1-2 per 1000 screens) particularly in women with dense breasts.
DBT Pros, Cons & Dose - Weighing the Options
- Pros:
- ↑ Cancer detection rates, especially for invasive cancers.
- ↓ Recall rates & false positives.
- Better lesion margin assessment & characterization.
- Improved visualization in dense breast tissue.
- Cons:
- ↑ Image acquisition time (longer compression).
- ↑ Radiologist interpretation time.
- Higher equipment cost.
- Potential for motion artifacts.
- Radiation Dose:
- DBT alone: Radiation dose is ~1.2 - 2.0 times that of 2D mammography.
- Combined 2D+DBT: Higher total dose if 2D acquired separately.
- Synthesized 2D (s2D) from DBT data can ↓ overall dose compared to separate 2D+DBT, making it comparable to 2D FFDM alone.
- Overall dose generally within acceptable regulatory limits (e.g., FDA single view average glandular dose limit <3 mGy).
- ⭐ > DBT significantly reduces patient recall rates, often by 15-40%, thereby decreasing unnecessary workups and patient anxiety associated with false positives.
High‑Yield Points - ⚡ Biggest Takeaways
- DBT (3D mammography) utilizes multiple low-dose X-ray projections acquired in an arc.
- Significantly reduces tissue overlap, improving lesion detection and characterization, especially in dense breasts.
- Increases cancer detection rate (CDR), particularly for invasive cancers.
- Decreases recall rates by clarifying findings ambiguous on 2D mammography.
- Synthesized 2D (s2D) images, generated from DBT data, can replace conventional 2D views, reducing overall radiation dose.
- Key limitations include longer acquisition time, potential for motion artifacts, and higher radiation dose if true 2D is also acquired.
- Superior for evaluating architectural distortions and focal asymmetries compared to 2D mammography alone.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more