

Short Stature: Definition & Triage - Height Checkpoint Alpha
- Definition: Height $ < \textbf{-2 SD}$ (Standard Deviations) below the mean, or $ < \textbf{3rd percentile}$ for the patient's chronological age and sex.
- Initial Evaluation:
- Accurate serial measurements (stadiometer/infantometer).
- Plot meticulously on appropriate growth charts (e.g., WHO, IAP).
- Calculate Mid-Parental Height (MPH) and projected target height range.
- Assess height velocity (crucial indicator).
- Triage Point: Is the short stature Proportionate or Disproportionate?
⭐ Mid-parental height calculation is crucial for differentiating familial short stature from pathological causes.

Loading diagram…
Short Stature: Etiology - Growth Mystery Files
| Category | Key Features / Examples |
|---|---|
| Normal Variants | |
| Familial Short Stature (FSS) | BA = CA; Normal growth velocity; Positive family history; Puberty normal. |
| Constitutional Delay (CDGP) | BA < CA; "Late bloomer"; Family history common; Puberty delayed; Normal adult height. |
| Pathological Causes | |
| Endocrine | GH Deficiency, Hypothyroidism, Cushing's, Precocious Puberty (early fusion). |
| Systemic Diseases | Malnutrition, CKD, Celiac, Cardiac, Pulmonary, Severe Anemia. |
| Genetic/Syndromic | Turner (XO), Down (Trisomy 21), Skeletal Dysplasias (Achondroplasia), Russell-Silver. |
| IUGR/SGA | Failure of catch-up growth. |
| Psychosocial | Emotional deprivation. |
| Iatrogenic | Chronic steroid use, Cranial irradiation. |
Short Stature: Clinical Evaluation - Height Detective Kit
- History Taking:
- Birth Hx (IUGR, SGA), Growth velocity (key!)
- Parental heights: Calculate Mid-Parental Height (MPH)
- Boys: $MPH = \frac{(Father's\ Ht + Mother's\ Ht + 13\ cm)}{2}$
- Girls: $MPH = \frac{(Father's\ Ht + Mother's\ Ht - 13\ cm)}{2}$
- Nutrition, Systemic illness, Psychosocial.
- Clinical Examination:
- Anthropometry: Ht (stadiometer), Wt, U/L ratio.
- Dysmorphism, Tanner stage.
- Investigations:
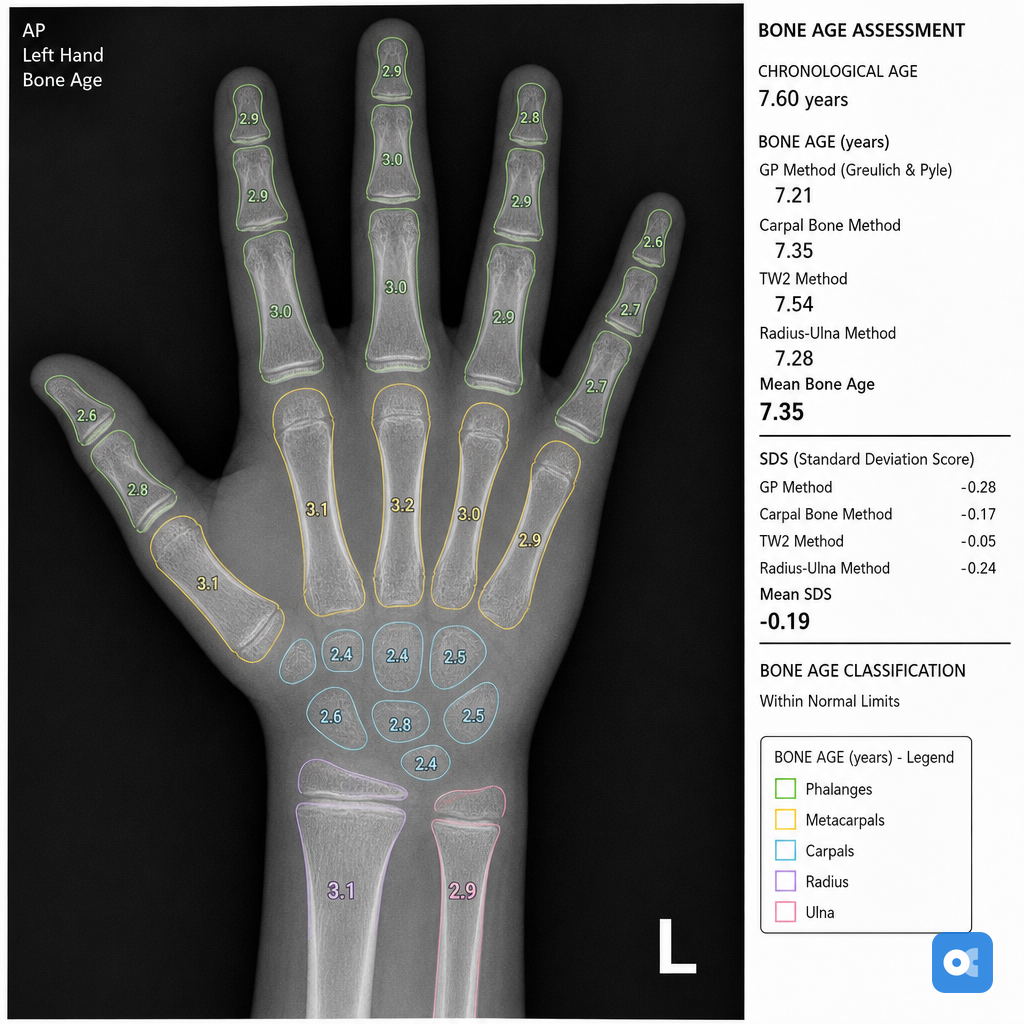
⭐ Bone age assessment (X-ray hand & wrist) is the single most useful initial investigation. It differentiates familial short stature (BA=CA) from constitutional delay or endocrine causes (BA<CA).
Loading diagram…
Short Stature: Syndromic Shorts - Tiny Titans Tales
Table: Syndromic Short Stature - Key Features
| Feature | Turner Syndrome | Achondroplasia | Growth Hormone Deficiency (GHD) |
|---|---|---|---|
| Genetics | $45,XO## Short Stature: Syndromic Shorts - Tiny Titans Tales |
Table: Syndromic Short Stature - Key Features
| FGFR3 mut (AD) | Various |
| Key Features | Webbed neck, shield chest, ovarian dysgenesis | Rhizomelic short, trident hand, macrocephaly | Proportional short, cherubic facies, delayed bone age | | Growth | ↓ velocity, no pubertal spurt | Disproportionate | ↓ velocity, proportional | | Assoc. | Coarctation (Ao), renal anomalies | Spinal stenosis | Hypoglycemia, delayed puberty | | Dx | Karyotype | Clinical, X-ray | GH stim tests, IGF-1 | | Rx | GH, Estrogen | Symptomatic | GH replacement |
⭐ Turner syndrome (karyotype 45,XO) is the most common syndromic cause of short stature in girls and is often associated with ovarian dysgenesis and congenital heart defects (e.g., coarctation of aorta).
High‑Yield Points - ⚡ Biggest Takeaways
- Short stature is height < -2 SD or < 3rd percentile for age and sex.
- Growth velocity is key; <4 cm/year (after age 4) suggests pathology.
- Bone age assessment is crucial; delayed in CDGP and hypothyroidism.
- Familial Short Stature (FSS): Normal bone age & velocity, matches Mid-Parental Height.
- CDGP: Delayed bone age & puberty, normal growth velocity, achieves normal adult height.
- Investigate pathological causes: Turner syndrome (girls), GH deficiency, chronic diseases.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more