

Acute and Chronic Inflammation - Body's Red Alert
- Inflammation: Protective response to injury.
- Acute Inflammation:
- Rapid onset, short duration.
- Cells: Neutrophils.
- Features: Exudation, edema.
- Chronic Inflammation:
- Slow onset, long duration.
- Cells: Lymphocytes, Macrophages.
- Features: Tissue destruction, fibrosis.
- Cardinal Signs (📌 PRISH):
- Pain (Dolor)
- Redness (Rubor)
- Immobility (Functio laesa)
- Swelling (Tumor)
- Heat (Calor)

⭐ The five cardinal signs of inflammation were first described by Celsus (calor, dolor, rubor, tumor), with functio laesa (loss of function) later added by Galen.
Acute and Chronic Inflammation - Rapid Firefighters
- Acute Inflammation: Rapid onset, short (days). Key cell: Neutrophil. Cardinal signs: Rubor, Tumor, Calor, Dolor, Functio laesa.
- Vascular: Vasodilation (NO, Histamine), ↑ Permeability (Histamine, Leukotrienes) → Exudate.
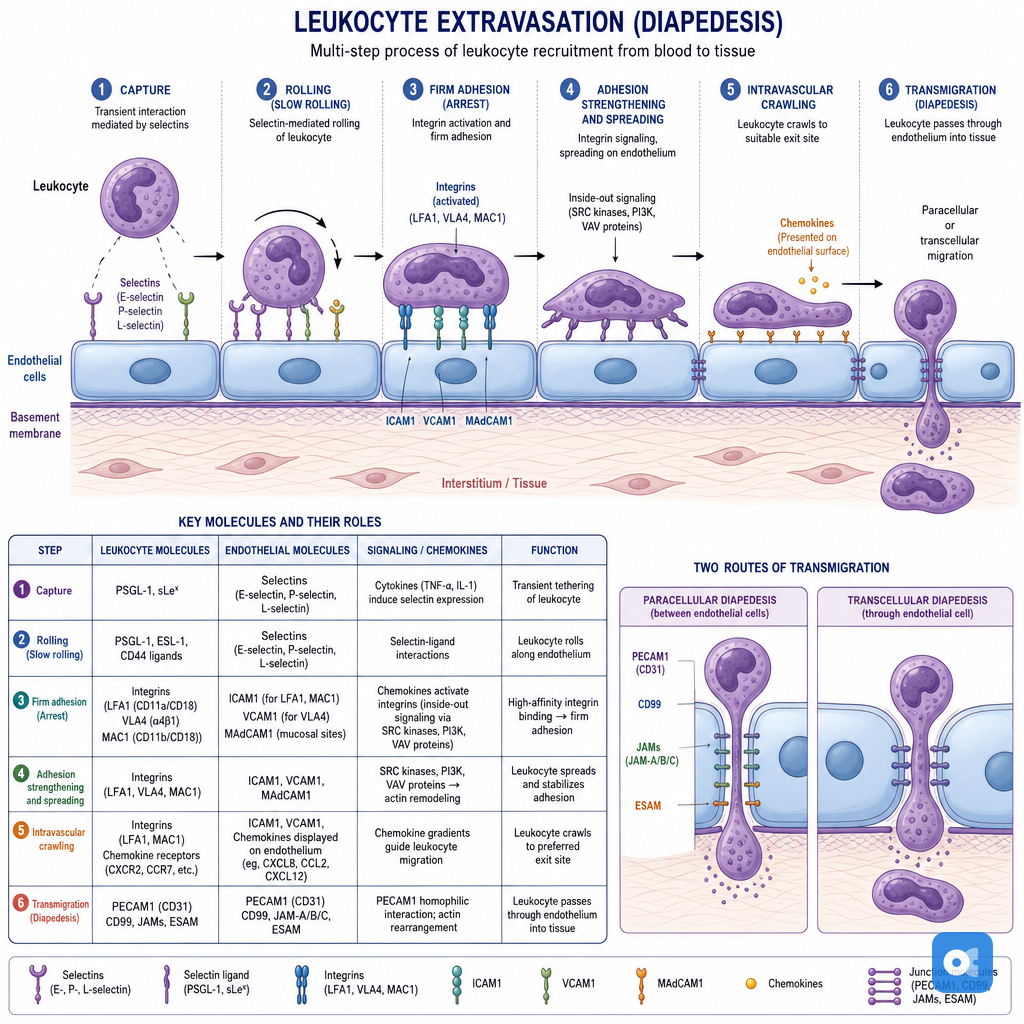
- Cellular: Leukocyte Extravasation (📌 'Margie Rolls Adhesively Trans Di Chemo')
Loading diagram…
- Phagocytosis: Opsonins (C3b, IgG). Killing: ROS, lysosomal enzymes.
- Key Mediators: TNF, IL-1, IL-6 (systemic), Chemokines (IL-8), Complement (C3a, C5a, C3b), AA metabolites (PGs, LTs).
- Outcomes: Resolution, Fibrosis, Abscess, or Chronic.
- Chronic Inflammation: Prolonged (weeks-months). Key cells: Lymphocytes, Macrophages. Tissue destruction & repair (angiogenesis, fibrosis) co-exist.
⭐ Defects in leukocyte adhesion (LAD type 1: LFA-1 integrin defect; LAD type 2: Sialyl-Lewis X defect) cause recurrent bacterial infections due to impaired neutrophil recruitment.
Acute and Chronic Inflammation - Chemical Signals & Scars
Chemical mediators (plasma/cell-derived) orchestrate vascular/cellular responses.
Key Chemical Mediators:
| Mediator | Source | Key Action(s) |
|---|---|---|
| Histamine | Mast cells, Basophils | Vasodilation, ↑ Vasc. permeability, Pruritus |
| Bradykinin | Plasma (Kinin system) | Vasodilation, ↑ Permeability, Pain |
| C3a, C5a | Plasma (Complement) | Mast cell degranulation; C5a: Chemotaxis, leukocyte activation |
| LTB₄ | Leukocytes | Chemotaxis, Neutrophil activation |
| PGE₂, PGD₂, PGI₂ | Mast cells, Endothelium | Vasodilation, Pain, Fever (PGE₂), Edema |
| TNF, IL-1 | Macrophages, Mast cells | Endothelial activation, Fever, Systemic effects |
| Chemokines (e.g. IL-8) | Macrophages, Endothelial cells | Leukocyte recruitment & activation |
| Nitric Oxide (NO) | Endothelium, Macrophages | Vasodilation, Microbicidal, ↓ Platelet agg. |
- Cell membrane phospholipids release AA, metabolized by COX & LOX.
- $AA \rightarrow Prostaglandins (PG), Leukotrienes (LT), Lipoxins (LX)$.
Complement System Activation: Activates via classical, alternative, or lectin pathways.
Loading diagram…
⭐ Prostaglandin E2 (PGE₂) mediates fever and pain in inflammation. (📌 Fever: IL-1, TNF, PGE₂)
Chronic Inflammation & Scarring:
- Persistent injury → chronic inflammation.
- Key mediators: Growth factors (TGF-β, PDGF from MΦ, lymphocytes) → fibroblast activation → collagen deposition → fibrosis (scar).
Acute and Chronic Inflammation - The Long War
- Chronic Inflammation: Prolonged; macrophages, lymphocytes, plasma cells. Tissue injury & repair (fibrosis, angiogenesis).
- Key Cells:
- Macrophages: Dominant. IFN-γ (classical activation), IL-4/IL-13 (alternative). Secrete TNF, IL-1.
- Lymphocytes: T & B cells; interact with macrophages.
- Granulomatous Inflammation: Epithelioid macrophages (activated), often with lymphocytes, Langhans giant cells.
- Granuloma Types:
Feature TB Sarcoidosis Foreign Body Cat Scratch Necrosis Caseous Non-caseating Non-caseating Stellate Giant Cells Langhans Langhans, Asteroid Foreign body Langhans Assoc. M.tb Schaumann bodies Inert material B. henselae
⭐ Caseating granulomas: TB. Non-caseating: Sarcoidosis, Crohn's.
- Systemic Effects (Acute Phase Response):
- Fever (IL-1, TNF → PGE₂). ↑CRP (<10 mg/L normal), ↑SAA, ↑Fibrinogen (↑ESR).
- Leukocytosis. Anemia of chronic disease (hepcidin).
High‑Yield Points - ⚡ Biggest Takeaways
- Acute inflammation: Characterized by neutrophils, exudation, and vasodilation. Key mediators: histamine, prostaglandins, leukotrienes.
- Chronic inflammation: Involves lymphocytes, macrophages, leading to tissue destruction and fibrosis.
- Cardinal signs of acute inflammation: Rubor, tumor, calor, dolor, functio laesa.
- Granulomatous inflammation: Features epithelioid macrophages and giant cells (e.g., Langhans).
- Tuberculosis shows caseating granulomas; sarcoidosis presents with non-caseating granulomas.
- Key cytokines: TNF and IL-1 drive acute inflammation; IFN-γ activates macrophages in chronic states.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more