

Blistering Basics - Bubble Trouble Intro
- Blister: Localized fluid collection within or below the epidermis.
- Vesicle: < 1 cm diameter.
- Bulla: > 1 cm diameter.
- Anatomical Levels of Cleavage (key to classification):
- Intraepidermal (within the epidermis):
- Subcorneal: Beneath stratum corneum.
- Intraspinous: Within stratum spinosum (acantholysis).
- Suprabasal: Above basal cell layer.
- Subepidermal (at/below Dermo-Epidermal Junction - DEJ):
- Lamina Lucida: Within upper basement membrane zone.
- Lamina Densa: Within middle basement membrane zone.
- Sub-Lamina Densa: Below lamina densa (anchoring fibril zone).
- Intraepidermal (within the epidermis):

⭐ The level of split is the most crucial initial step in classifying blistering diseases.
Intraepidermal Blisters - Skin's Inner Strife
-
Mechanism: Acantholysis (loss of keratinocyte adhesion). Autoantibodies target Desmogleins.
-
Clinical: Flaccid blisters, Nikolsky sign positive (epidermal separation on pressure).
-
DIF: Intercellular 'chicken-wire' IgG & C3 deposits.
-
Key Types:
- Pemphigus Vulgaris (PV):
- Targets: Dsg3 (mucosa/skin) ± Dsg1 (skin).
- Clinical: Oral erosions (80-90%), flaccid skin blisters; deeper split.
- Pemphigus Foliaceus (PF):
- Target: Dsg1 only (superficial epidermis).
- Clinical: Scaly, crusted erosions; no mucosal involvement. Fogo Selvagem form.
- IgA Pemphigus: IgA deposits; neutrophilic pustules.
- Paraneoplastic Pemphigus: Malignancy-associated; severe stomatitis, polymorphic lesions.
- Pemphigus Vulgaris (PV):
📌 Mnemonic: Vulgaris = Very deep (Dsg3); Foliaceus = Flakes (superficial Dsg1).
⭐ Pemphigus vulgaris commonly affects oral mucosa (80-90%) and skin; Pemphigus foliaceus spares mucous membranes.
Subepidermal Blisters - Dermal Divide Drama
- Mechanism: Immune attack on dermoepidermal junction (DEJ) structural components → separation below epidermis, forming tense blisters. 📌 'B'P = 'B'asement membrane, 'B'elow.
- Key Diseases & Features:
| Disease | Antigen(s) | DIF | Clinical |
|---|---|---|---|
| Bullous Pemphigoid (BP) | BPAG1 (BP230), BPAG2 (BP180) | Linear IgG/C3 at BMZ | Elderly, tense subepidermal bullae, intense pruritus, Nikolsky usually negative. |
| Dermatitis Herpetiformis (DH) | Epidermal/Tissue Transglutaminase (eTG/tTG) | Granular IgA in dermal papillae | Intensely pruritic grouped vesicles (extensors), strong celiac disease association. |
| Epidermolysis Bullosa Acquisita (EBA) | Type VII collagen | Linear IgG/C3 at BMZ (dermal side salt-split) | Trauma-induced non-inflammatory blisters, acral distribution, heals with scarring & milia. |
| Linear IgA Bullous Dermatosis (LABD) | LAD-1 (cleaved BPAG2), LABD97 | Linear IgA at BMZ | Children/adults, annular or "string of pearls" vesicles/bullae. |
| Cicatricial Pemphigoid | BP180, Laminin-332, Type VII collagen | Linear IgG/C3/IgA at BMZ | Chronic, mainly mucosal (oral, ocular) blisters with progressive scarring. |
| Pemphigoid Gestationis | BP180 (BPAG2) | Linear C3 (± IgG) at BMZ | Pregnancy (2nd/3rd trimester)/postpartum, pruritic urticarial papules/plaques then blisters, often periumbilical. |
Diagnostic Approach - Skin Sleuth Central
- Key Investigations:
- Skin Biopsy: H&E (split level, infiltrate); DIF (perilesional, gold standard for immune deposits).
- IIF (Serum): Detects circulating autoantibodies (substrates: monkey esophagus, salt-split skin).
- ELISA: Quantifies specific autoantibodies (e.g., Dsg1, Dsg3, BP180, BP230).
- Tzanck Smear: Herpes (multinucleated giant cells); Pemphigus (acantholytic cells).
- Nikolsky Sign: Clinical indicator of epidermal fragility.
- Diagnostic Flow:
Loading diagram…
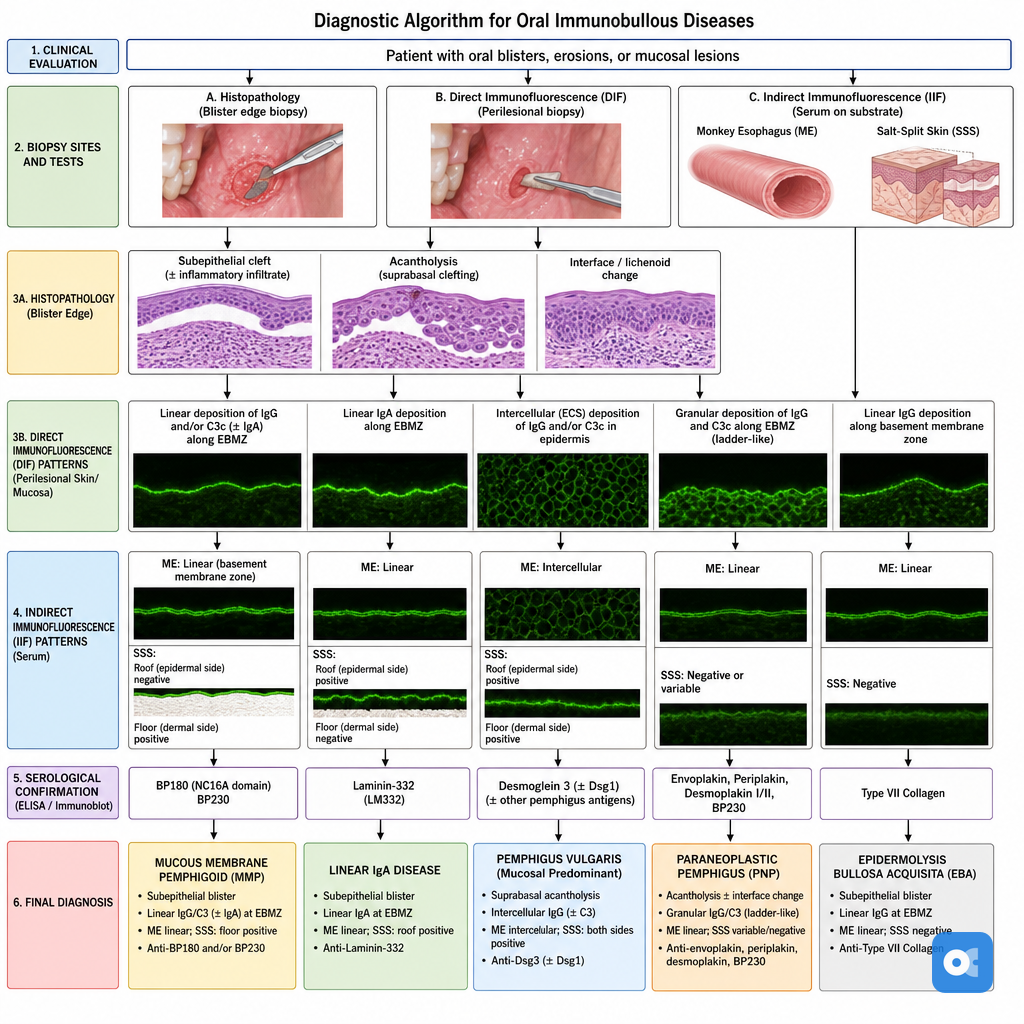
⭐ Salt-split skin immunofluorescence is crucial: in Bullous Pemphigoid, antibodies bind to the roof (epidermal side) of the split, while in Epidermolysis Bullosa Acquisita, they bind to the floor (dermal side).
High‑Yield Points - ⚡ Biggest Takeaways
- Pemphigus vulgaris: Intraepidermal bullae due to acantholysis; Nikolsky positive; targets Desmoglein 3 & 1.
- Bullous pemphigoid: Subepidermal, tense blisters; Nikolsky negative; targets hemidesmosomal proteins (BPAG1/BPAG2).
- Dermatitis herpetiformis: Subepidermal with neutrophilic papillary microabscesses; IgA deposits; strong celiac disease link.
- Epidermolysis bullosa: Inherited mechanobullous disorders; blisters from minor trauma; variable cleavage planes.
- Pemphigus foliaceus: More superficial intraepidermal (subcorneal) blisters; targets Desmoglein 1 primarily.
- Linear IgA Bullous Dermatosis (LABD): Subepidermal blisters with linear IgA deposition along the basement membrane zone.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more