

Limb Length Discrepancies - Uneven Steppers
- Definition: Limb Length Discrepancy (LLD) is a condition characterized by a clinically significant difference in the length of corresponding limbs.
- Types of LLD:
- True LLD: An actual anatomic shortening of one or more bones in the limb.
- Apparent LLD: Limbs have equal bony lengths, but appear unequal due to factors like joint contractures (hip, knee, ankle) or fixed pelvic obliquity.
Common Etiologies:
| Category | Examples |
|---|---|
| Congenital | Hemihypertrophy (overgrowth of one side of body), Fibular hemimelia (partial/complete absence of fibula) |
| Acquired | Physeal injury (growth plate damage), Infection (e.g., osteomyelitis), Bone tumors, Neuromuscular disorders (e.g., cerebral palsy, polio) |
Limb Length Discrepancies - Measure Up!
-
History (Key Clues)
- Birth: Congenital (e.g., hemihypertrophy, fibular hemimelia)
- Trauma: Physeal injury
- Infection: Osteomyelitis, septic arthritis affecting physis
-
Physical Examination
- Galeazzi test (Allis sign): Observe knee height (supine, hips & knees flexed) for femoral vs. tibial LLD.
- Block test: Place calibrated blocks under shorter limb until iliac crests level; quantifies LLD.
- Assess for: Pelvic obliquity, compensatory/functional scoliosis, Trendelenburg gait.
- Differentiate: True LLD (measure ASIS to medial malleolus) vs. Apparent LLD (due to adduction/abduction contractures, pelvic asymmetry).

-
Measurement Techniques
Technique Accuracy Radiation Notes Tape Measure ↓ None Screening; high inter-observer variability Orthoroentgenogram Moderate Moderate Single long film; prone to magnification error Scanogram ↑ ↓ Multiple focused X-rays over joints with ruler CT Scanogram Highest Moderate Gold Standard; precise, 3D assessment
⭐ CT scanogram is considered the gold standard for accurate LLD measurement, especially for complex cases or when surgical planning is required.
Limb Length Discrepancies - Treat or Wait?
Key considerations for management. Consequences of untreated LLD: - Gait abnormalities (e.g., Trendelenburg) - Chronic back pain - Functional scoliosis - Premature hip/knee Osteoarthritis (OA) Growth prediction uses Moseley straight line graph or Anderson-Green charts.
⭐ Projected LLD at skeletal maturity is crucial for planning treatment in growing children; Moseley charts aid this.
Management algorithm:
Loading diagram…
Limb Length Discrepancies - Bridging Gaps
- Non-operative: Shoe lift (for < 2 cm discrepancy).
- Operative Options:
| Modality | Indications (LLD) | Adv. / Disadv. / Techniques | Max Correction |
|---|---|---|---|
| Epiphysiodesis | 2-5 cm (immature) | Simple (Phemister, percut.); Timing crucial | 2-5 cm |
| Limb Shortening | 2-6 cm (mature) | Osteotomy; Rapid recovery; ↓ height, muscle weak. | ~5-6 cm |
| Limb Lengthening | >5 cm (or 2-5 cm) | Restores height; Complex, ↑ complications, long Tx | 20-25% of bone length |
- Techniques: Ilizarov, ISKD, Precice.
- Rate: $1 \text{ mm/day}$ (e.g., **0.25 mm** QID).
- Consolidation Index: Healing duration/cm.
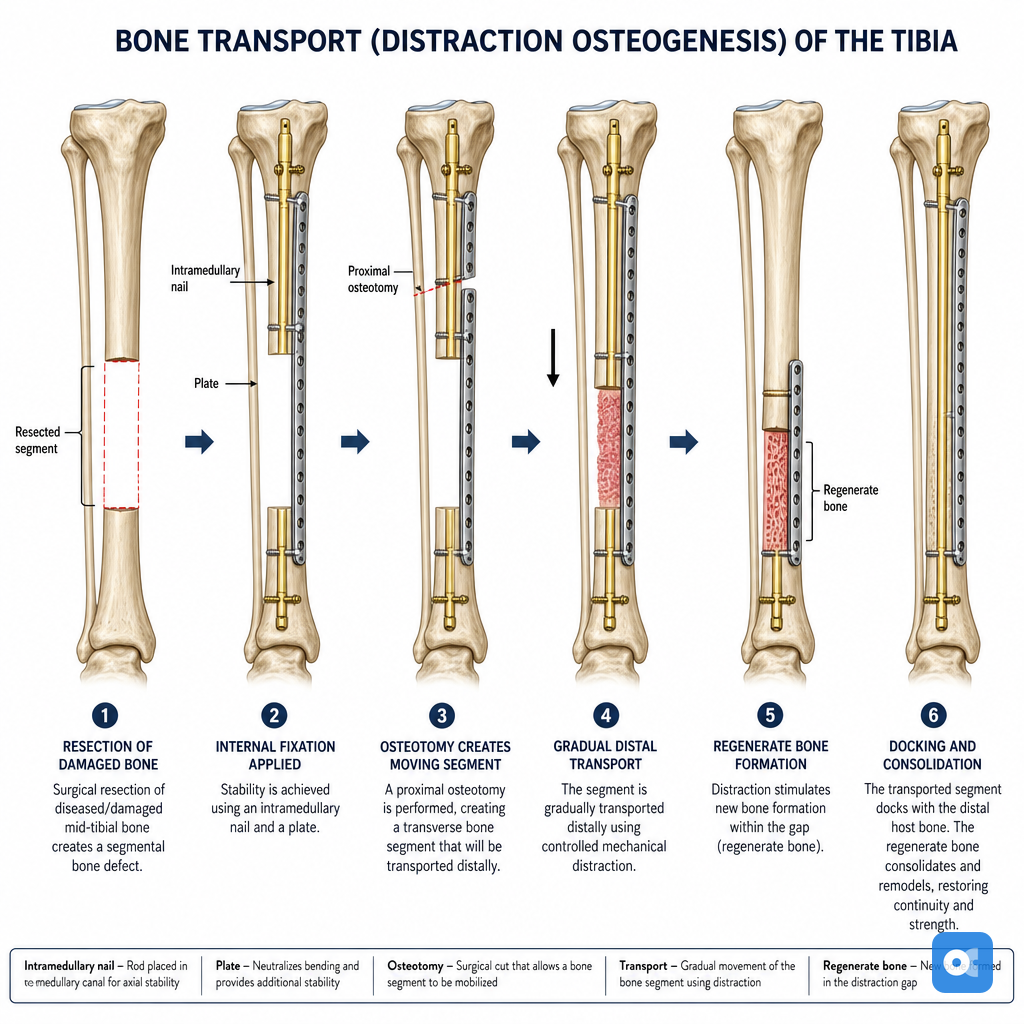
- Complications: Pin tract infection, joint stiffness, nonunion, nerve injury, premature/delayed consolidation.
⭐ The law of tension-stress (Ilizarov principle) is fundamental to successful limb lengthening by distraction osteogenesis.
High‑Yield Points - ⚡ Biggest Takeaways
- Limb Length Discrepancy (LLD) >2-2.5 cm is generally considered clinically significant, often requiring intervention.
- Common etiologies include congenital anomalies (e.g., fibular hemimelia), physeal injury (trauma, infection), tumors, and neuromuscular conditions.
- Accurate measurement using scanogram or CT scanogram is crucial; always assess skeletal maturity.
- Management strategy depends on magnitude and growth remaining: shoe lift (<2 cm), epiphysiodesis (2-5 cm with growth potential), or limb lengthening (>5 cm).
- Ilizarov technique (distraction osteogenesis) is a key method for significant limb lengthening.
- Potential complications of lengthening procedures include pin-tract infections, joint contractures/stiffness, and neurovascular injury.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more