

Overview & Pre-op - Setting Eye Stage
- Anesthesia Goals: Akinesia, analgesia, stable intraocular pressure (IOP), patient & surgeon comfort, minimize oculo-cardiac reflex (OCR).
- Pre-operative Evaluation:
- Thorough history: Systemic diseases (DM, HTN, asthma, bleeding disorders), medications (anticoagulants!), allergies, prior anesthesia experience.
- Ocular exam: Visual acuity, IOP, axial length (AL).
- Systemic exam: Airway, cardiovascular, respiratory.
- Investigations: Guided by ASA status & co-morbidities (ECG, blood sugar, coagulation profile if needed).
- Patient Preparation:
- Informed consent: Discuss technique, risks (e.g., retrobulbar hemorrhage, globe perforation), benefits.
- Fasting: NPO ~6 hrs for solids, ~2 hrs for clear fluids.
- Premedication: Anxiolytics (e.g., Diazepam 5-10 mg oral / Midazolam 1-2 mg IV), antiemetics if high risk.
⭐ For patients on anticoagulants/antiplatelets (e.g., Warfarin, Aspirin, Clopidogrel), individualized decision on stopping/bridging (typically 5-7 days prior for Aspirin) balancing thrombotic vs. bleeding risk is crucial.

Local Anesthesia Types - Eye Block Party
-
Topical: Proparacaine 0.5%, Tetracaine 0.5-1%. For minor procedures. Rapid onset, short duration.
-
Infiltrative:
- Subconjunctival: Chalazion, pterygium.
- Sub-Tenon's (Episcleral): Cannula for posterior block. Good akinesia, safer.
-
Regional Needle Blocks:
- Retrobulbar (Intraconal):
- Targets ciliary ganglion, CN II, III, VI. Volume: 3-5 mL.
- Rapid, dense block. Risks: Globe perforation, RBH, optic nerve injury.
- Peribulbar (Extraconal):
- Larger volume: 6-12 mL. Safer than retrobulbar.
- Slower onset, more chemosis.
- Facial Nerve Blocks: Van Lint (periorbital), O'Brien (truncal). For eyelid akinesia.
- Retrobulbar (Intraconal):
⭐ Hyaluronidase (5-7 IU/mL) added to LA enhances spread & onset.
Anesthetic Agents & Mixes - Potion Power-Ups
- Local Anesthetics (LAs):
- Amides (Low allergy risk):
- Lignocaine (Xylocaine): Rapid onset, 1-2 hr duration. Max: 4.5 mg/kg (plain), 7 mg/kg (w/ adrenaline).
- Bupivacaine (Sensorcaine): Slow onset, 4-8 hr duration. Highly cardiotoxic. Max: 2 mg/kg.
- Ropivacaine: Similar to bupivacaine, less cardiotoxic.
- Esters (e.g., Procaine): Higher allergy risk (PABA metabolite).
- Amides (Low allergy risk):
- Adjuvants:
- Adrenaline: Vasoconstrictor. ↑duration, ↓toxicity, ↓bleeding. Conc: 1:100,000-1:200,000.
- Hyaluronidase: Spreading factor. ↑diffusion. Dose: 5-15 IU/mL.
- Sodium Bicarbonate: Alkalinization. Speeds LA onset by ↑non-ionized form.
- Common Mix (Retrobulbar): Lignocaine + Bupivacaine + Hyaluronidase ± Adrenaline.
⭐ Bupivacaine is highly cardiotoxic; lipid emulsion is the antidote for LA systemic toxicity (LAST).
GA & Complications - Risky Eye Business
- General Anesthesia (GA) Indications: Pediatrics, long surgery (>2 hrs), patient refusal local, open globe, uncooperative.
- Agents: Propofol, Sevoflurane (all ↓IOP). Avoid Ketamine (↑IOP). LMA preferred over ETT (↓coughing, ↓IOP).
- Complications (Local & GA):
- Oculocardiac Reflex (OCR): 📌 "Five (V) & Dime (X)" (Trigemino-vagal). Bradycardia from EOM traction. Mgmt: Stop stimulus, Atropine 0.01-0.02 mg/kg IV.
Loading diagram…
- **Retrobulbar Hemorrhage (RBH):** Proptosis, ↑IOP, diplopia. Mgmt: Lateral canthotomy & cantholysis (immediate).
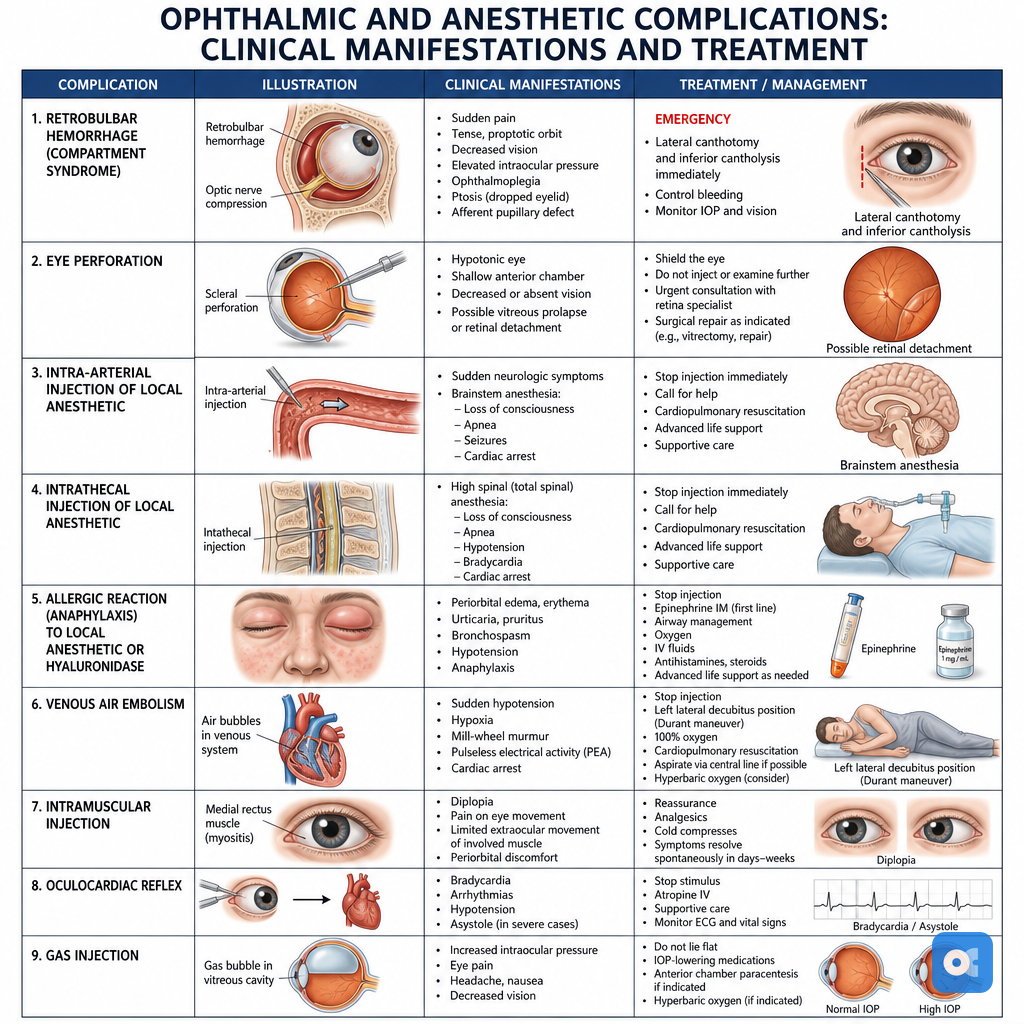
- Globe Perforation: Pain, ↓vision, hypotony. Risk ↑ high myopia (long axial length).
- Brainstem Anesthesia (Retrobulbar): Apnea, LOC, seizures. Mgmt: Airway support.
- Malignant Hyperthermia (GA: Succinylcholine/inhalational agents).
- PONV common.
⭐ Oculocardiac reflex is most common with medial rectus muscle traction during strabismus surgery.
High‑Yield Points - ⚡ Biggest Takeaways
- Retrobulbar block (RBB): Most common, akinesia, anesthesia. Risks: hemorrhage, perforation.
- Peribulbar block: Safer than RBB, larger volume, slower onset. Lower perforation risk.
- Sub-Tenon's block: For glaucoma surgery, minimal IOP rise, limited akinesia.
- Topical anesthesia: For anterior segment surgery (phaco). Proparacaine, lignocaine.
- General anesthesia (GA): For children, uncooperative adults, long surgeries, open globe injuries.
- Oculocardiac reflex (OCR): EOM traction → bradycardia. Manage with atropine.
- Hyaluronidase: Added to LA to enhance spread, ↓ orbital pressure.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more