
Oculoplasty

On this page
👁️ Oculoplasty: The Periocular Reconstruction Mastery
Oculoplasty sits at the crossroads of ophthalmology, plastic surgery, and systemic medicine, demanding mastery of delicate periocular anatomy, biomechanics, and reconstructive principles that protect both function and appearance. You'll build a systematic approach from foundational architecture through clinical pattern recognition, differential diagnosis, and evidence-based interventions, learning to navigate complex cases where eyelid malposition, orbital pathology, and lacrimal disorders intersect with broader medical conditions. This lesson equips you with the clinical reasoning framework and treatment algorithms to confidently diagnose and manage the full spectrum of periocular disease.
👁️ Oculoplasty: The Periocular Reconstruction Mastery

🏗️ Section 1 - The Periocular Architecture: Foundation Blueprint
The periocular region encompasses 7 distinct anatomical layers in the eyelid alone, each serving critical protective and functional roles. The anterior lamella consists of skin (0.5mm thick) and orbicularis oculi muscle, while the posterior lamella includes the tarsal plate (1mm thick in upper lid, 0.5mm in lower lid) and conjunctiva.
📌 Remember: STOP for eyelid layers - Skin, Tarsal plate, Orbicularis oculi, Posterior conjunctiva. Each layer requires specific surgical consideration during reconstruction procedures.
- Orbital Septum Architecture
- Upper lid: Fuses with levator aponeurosis 3-5mm above tarsal border
- Lower lid: Fuses with capsulopalpebral fascia 5mm below tarsal border
- Clinical significance: Determines fat pad herniation patterns
- Surgical landmark: Critical for blepharoplasty approaches
- Tarsal Plate Dimensions
- Upper tarsus: 10-12mm height, 29mm width
- Lower tarsus: 4-5mm height, 29mm width
- Contains 25-40 meibomian glands in upper lid
- Contains 20-30 meibomian glands in lower lid
| Structure | Upper Lid | Lower Lid | Clinical Significance | Surgical Considerations | Pathological Changes |
|---|---|---|---|---|---|
| Tarsal Height | 10-12mm | 4-5mm | Lid stability | Reconstruction limits | Cicatricial shortening |
| Fat Compartments | 2 (nasal, central) | 3 (nasal, central, temporal) | Herniation patterns | Blepharoplasty approach | Age-related prolapse |
| Meibomian Glands | 25-40 | 20-30 | Tear film stability | Preservation priority | MGD complications |
| Muscle Thickness | 0.5-1mm | 0.3-0.5mm | Closure strength | Suture placement | Denervation atrophy |
| Conjunctival Zones | Tarsal, forniceal | Tarsal, forniceal | Mucin production | Graft donor sites | Cicatricial changes |
The neurovascular supply demonstrates remarkable redundancy, with dual arterial arcades in the upper lid (marginal and peripheral) ensuring robust perfusion during surgical manipulation. The facial nerve's temporal and zygomatic branches provide motor innervation with cross-innervation patterns that explain partial recovery in facial palsy cases.
💡 Master This: Every oculoplastic procedure depends on understanding the anterior vs posterior lamella concept. Anterior lamella defects require skin-muscle grafts, while posterior lamella defects need tarsoconjunctival reconstruction. Mixed defects demand staged procedures with 6-8 week intervals.
- Critical Measurements for Surgical Planning
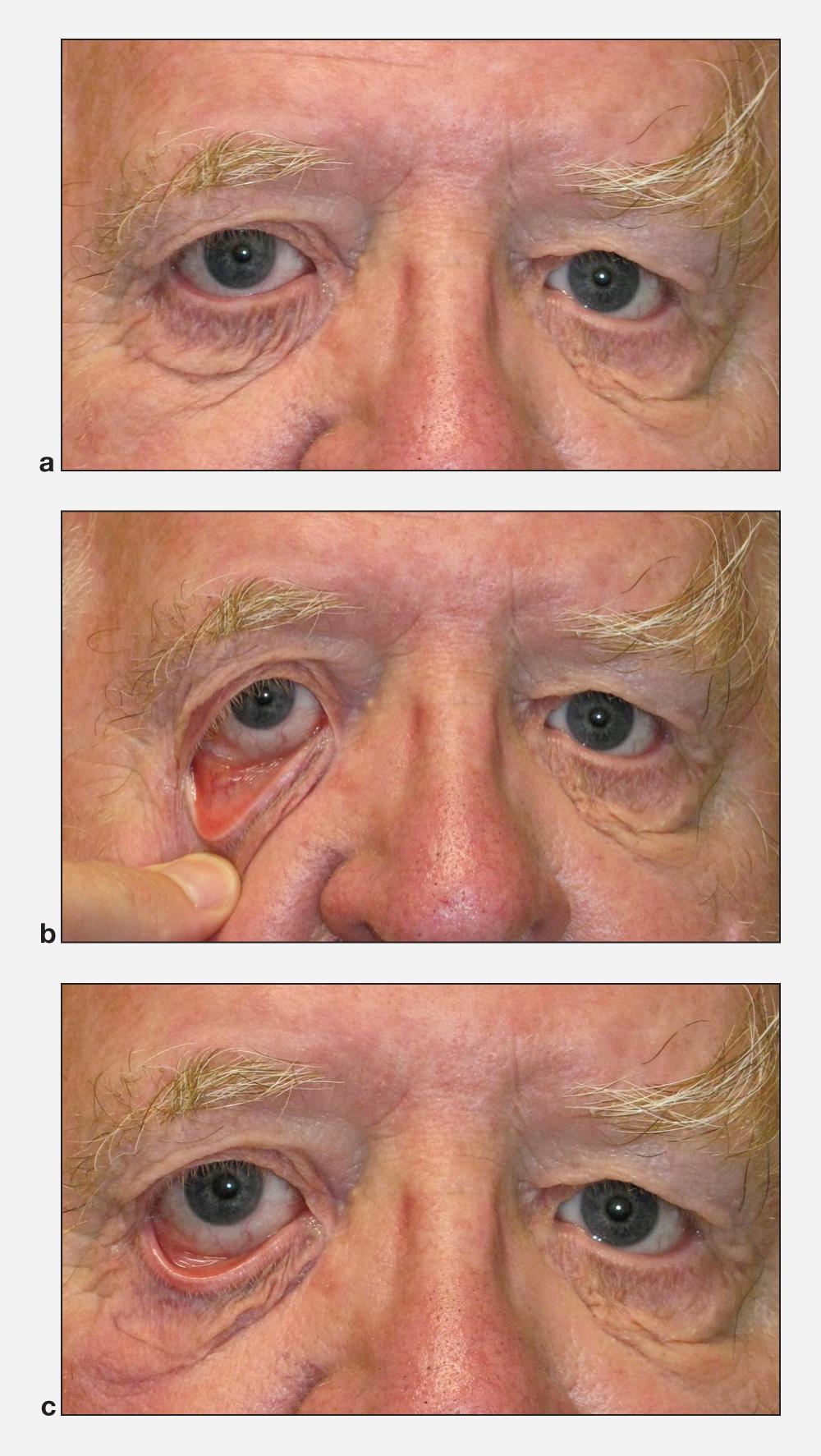
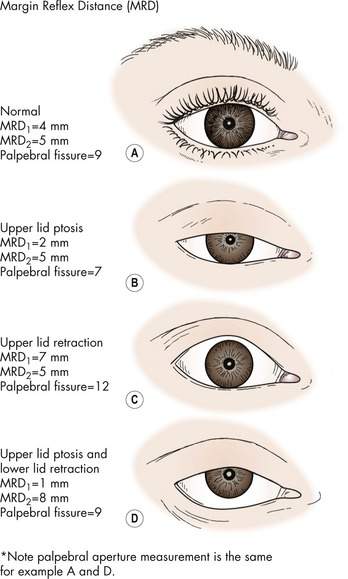
- Marginal reflex distance 1 (MRD1): 4-5mm (upper lid to corneal light reflex)
- Marginal reflex distance 2 (MRD2): 5-6mm (lower lid to corneal light reflex)
- Palpebral fissure height: 9-12mm in primary gaze
- Interpalpebral distance: 28-30mm horizontally
- Medial canthal angle: 48-52 degrees
- Lateral canthal angle: 60-65 degrees
Understanding these foundational relationships enables precise surgical planning and predicts functional outcomes across all oculoplastic procedures.
🏗️ Section 1 — The Periocular Architecture: Foundation Blueprint

⚙️ Section 2 - The Biomechanical Engine: Functional Dynamics Decoded
Loading diagram…
📌 Remember: LIFT mechanism - Levator contracts, Insertion via aponeurosis, Functional elevation, Tarsal attachment. Failure at any point creates specific ptosis patterns with distinct surgical requirements.
The blinking mechanism operates through dual motor systems: voluntary (cortical) and involuntary (brainstem). Spontaneous blinks occur every 3-4 seconds with 300-400ms duration, generating 5-7mmHg pressure to distribute 7-10 microliters of tear film across the corneal surface.
- Biomechanical Force Vectors
- Levator muscle: Primary elevator with 15g lifting force
- Müller's muscle: Secondary elevator with 2-3mm sympathetic contribution
- Innervation: Sympathetic fibers from superior cervical ganglion
- Clinical correlation: Horner's syndrome causes 1-2mm ptosis
- Orbicularis oculi: Closure mechanism with orbital and palpebral divisions
- Orbital portion: Forceful closure (20-30g pressure)
- Palpebral portion: Gentle closure (5-10g pressure)
| Muscle Component | Force Generated | Excursion Range | Innervation | Failure Pattern | Surgical Approach |
|---|---|---|---|---|---|
| Levator Palpebrae | 15-20g | 15-20mm | CN III | Aponeurotic ptosis | Aponeurosis repair |
| Müller's Muscle | 2-3g | 2-3mm | Sympathetic | Horner's ptosis | Conjunctival-Müller resection |
| Orbicularis (Orbital) | 20-30g | 5-8mm | CN VII | Lagophthalmos | Lid loading/tightening |
| Orbicularis (Palpebral) | 5-10g | 2-3mm | CN VII | Incomplete closure | Gold weight implant |
| Superior Rectus | 8-12g | 10-15mm | CN III | Ptosis with gaze restriction | Combined approach |
The tear film distribution mechanism requires precise lid-globe apposition with 2-3mmHg capillary pressure. Disruption of this relationship through ectropion or entropion creates exponential increases in tear film instability, with >4mm lid malposition causing 90% reduction in tear film stability.
💡 Master This: Biomechanical failure follows predictable patterns based on the weakest link principle. Aponeurotic dehiscence occurs at tarsal insertion in 75% of age-related ptosis, while traumatic ptosis typically involves muscle belly damage requiring different surgical strategies.
- Age-Related Biomechanical Changes
- Aponeurotic stretching: 0.5mm annually after age 40
- Tarsal plate thinning: 10-15% reduction per decade
- Orbicularis muscle weakness: 2-3% force reduction annually
- Collagen cross-linking: Decreased elasticity 20-30%
- Neural conduction: Slowed by 5-10% per decade
- Fascial support: Weakened by 15-25% over lifetime
Understanding these biomechanical principles enables precise diagnosis of functional deficits and guides appropriate surgical intervention timing and technique selection.
⚙️ Section 2 — The Biomechanical Engine: Functional Dynamics Decoded


🎯 Section 3 - The Clinical Recognition Matrix: Pattern Mastery Framework
📌 Remember: MEASURE for ptosis evaluation - MRD1 measurement, Excursion testing, Aponeurosis function, Symmetry assessment, Upper lid crease, Reflex testing, Eye movement evaluation. Each component provides critical diagnostic information.
- Ptosis Recognition Patterns
- Aponeurotic ptosis: High lid crease (>8mm), good levator function (>12mm)
- Myogenic ptosis: Normal crease (6-8mm), poor levator function (<8mm)
- Congenital: Absent crease, minimal excursion (<4mm)
- Myasthenic: Variable measurements, fatigue testing positive
- Neurogenic ptosis: Associated extraocular muscle weakness, pupil involvement
- CN III palsy: Complete ptosis, dilated pupil, limited eye movement
- Horner's syndrome: Mild ptosis (1-2mm), miosis, anhidrosis
Loading diagram…
| Ptosis Type | MRD1 | Levator Function | Lid Crease | Associated Signs | Surgical Success Rate |
|---|---|---|---|---|---|
| Aponeurotic | <2mm | >12mm | >8mm | Age-related changes | >95% |
| Congenital | Variable | <8mm | Absent/Low | Jaw-winking possible | 85-90% |
| Myasthenic | Variable | Fatigable | Normal | Cogan's sign positive | Medical management |
| CN III Palsy | Complete | 0mm | Normal | EOM limitation, pupil | Poor without nerve recovery |
| Horner's | 1-2mm | >12mm | Normal | Miosis, anhidrosis | >90% with Müller resection |
Lid Malposition Recognition Framework:
- Ectropion Patterns
- Involutional: Lower lid laxity, >6mm distraction test
- Cicatricial: Skin shortage, <4mm pinch test
- Snap-back test: >2 seconds indicates significant laxity
- Lateral canthal tendon laxity: >2mm lateral distraction
- Paralytic: Facial nerve weakness, incomplete closure
- Bell's phenomenon: Protective upward eye rotation
- Lagophthalmos: >2mm gap during gentle closure

💡 Master This: The lateral canthal angle normally measures 60-65 degrees. Angles >70 degrees indicate lateral canthal tendon laxity requiring surgical tightening, while angles <55 degrees suggest overcorrection or cicatricial changes.
- Entropion Recognition Criteria
- Spastic: Orbicularis spasm, temporary with anesthesia
- Involutional: Horizontal laxity plus retractor dehiscence
- Lower lid retractor weakness: <3mm inferior excursion
- Tarsal plate instability: Inward rotation with gentle pressure
- Cicatricial: Posterior lamella shortage, permanent inversion
- Conjunctival scarring: Visible fibrosis and shortening
- Fornix foreshortening: <8mm depth measurement
Understanding these recognition patterns enables rapid diagnosis within 30-60 seconds of clinical examination, immediately directing appropriate treatment algorithms and surgical planning considerations.
🎯 Section 3 — The Clinical Recognition Matrix: Pattern Mastery Framework


🔬 Section 4 - The Differential Diagnosis Engine: Systematic Discrimination Mastery
📌 Remember: DISCRIMINATE for lid malposition - Distraction testing, Inversion assessment, Snap-back timing, Canthal angle measurement, Retractor function, Inflammation signs, Muscle tone, Innervation testing, Normal vs abnormal, Age-related changes, Tissue quality, Excursion measurement.
- Ptosis Differential Framework
- Measurement-Based Discrimination
- Levator function >12mm: Aponeurotic (85% probability)
- Levator function 4-8mm: Mixed aponeurotic-myogenic
- Levator function <4mm: Myogenic (90% probability)
- Associated Sign Patterns
- Jaw-winking: Marcus Gunn syndrome (5% of congenital ptosis)
- Fatigue testing: Myasthenia gravis (2-3% of ptosis cases)
- Pupil involvement: CN III palsy (<1% of ptosis presentations)
- Measurement-Based Discrimination
| Discriminating Feature | Aponeurotic | Congenital | Myasthenic | Neurogenic | Mechanical |
|---|---|---|---|---|---|
| Age of Onset | >40 years | Birth | 20-50 years | Variable | Post-trauma |
| Levator Function | >12mm | <8mm | Variable | <4mm | Variable |
| Lid Crease Height | >8mm | Absent | Normal | Normal | Distorted |
| Diurnal Variation | None | None | Marked | None | None |
| Response to Rest | None | None | Improvement | None | None |
| Bilateral Involvement | Common | 25% | >80% | Variable | Rare |
| Family History | Rare | Common | 10% | Rare | None |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | |||||
| flowchart TD |
Start["👁️ Ptosis Assessment
• Eyelid drooping• Subjective history"]
Age["📋 Age of Onset
• Birth vs later• Crucial first step"]
Cong["🩺 Congenital
• Present at birth• Evaluation phase"]
Acq["🩺 Acquired
• Adult onset• New symptoms"]
Lev["📋 Levator Function
• Muscle strength• Measure ⬇️ excursion"]
SevC["✅ Severe Congenital
• Less than 4mm• Surgical priority"]
ModC["✅ Moderate
• 4 to 8mm travel• Congenital type"]
Diur["📋 Diurnal Variation
• Worse later today• Fatigue effect"]
MG["🔬 Myasthenia Test
• Tensilon or Ice• Check antibodies"]
Pupil["📋 Pupil Involved
• Check symmetry• Horner vs CN III"]
Neuro["🔬 Neuro Workup
• Imaging needed• Nerve assessment"]
Apon["✅ Aponeurotic
• Muscle dehiscence• Common in aging"]
Start --> Age Age -->|Birth| Cong Age -->|Adult| Acq Cong --> Lev Lev -->|LT 4mm| SevC Lev -->|4-8mm| ModC Acq --> Diur Diur -->|Yes| MG Diur -->|No| Pupil Pupil -->|Yes| Neuro Pupil -->|No| Apon
style Start fill:#EEFAFF, stroke:#DAF3FF, stroke-width:1.5px, rx:12, ry:12, color:#0369A1 style Age fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style Cong fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style Acq fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style Lev fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style SevC fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252 style ModC fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252 style Diur fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style MG fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C style Pupil fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style Neuro fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C style Apon fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252
> ⭐ **Clinical Pearl**: **Cogan's lid twitch sign** demonstrates **90% sensitivity** for myasthenia gravis. After sustained downgaze for **15 seconds**, rapid return to primary position shows **brief overshoot** followed by gradual ptosis development in myasthenic patients.
**Ectropion vs Entropion Discrimination**:
* **Quantitative Differentiation Criteria**
- **Horizontal lid laxity**: Distraction **>6mm** indicates surgical intervention need
- **Snap-back test**: **>2 seconds** confirms significant laxity
+ Normal: **<1 second** return to globe
+ Mild laxity: **1-2 seconds** return
+ Severe laxity: **>3 seconds** or no spontaneous return
- **Lateral canthal tendon**: **>2mm** distraction indicates dehiscence
* **Cicatricial vs Involutional Discrimination**
- **Pinch test**: **<4mm** skin mobility suggests cicatricial component
- **Forced duction**: Resistance indicates cicatricial restriction
+ Involutional: Free movement with correction
+ Cicatricial: Persistent restriction despite manipulation
- **Conjunctival assessment**: Visible scarring confirms cicatricial etiology
| Discriminating Test | Normal Value | Mild Abnormal | Severe Abnormal | Clinical Significance |
|---------------------|--------------|---------------|-----------------|----------------------|
| Horizontal Distraction | **<4mm** | **4-6mm** | **>6mm** | Surgical indication threshold |
| Snap-back Time | **<1 second** | **1-2 seconds** | **>2 seconds** | Laxity severity grading |
| Lateral Distraction | **<1mm** | **1-2mm** | **>2mm** | Canthal tendon integrity |
| Pinch Test | **>8mm** | **4-8mm** | **<4mm** | Skin shortage assessment |
| Lower Lid Excursion | **>5mm** | **3-5mm** | **<3mm** | Retractor function evaluation |> 💡 **Master This**: The **forced duction test** differentiates mechanical restriction from muscle weakness with **>95% accuracy**. Positive resistance during passive movement indicates cicatricial changes requiring different surgical approaches than simple muscle weakness or laxity.
Understanding these discrimination criteria enables **definitive diagnosis** within **2-3 minutes** of systematic examination, immediately directing appropriate treatment algorithms and preventing misdiagnosis-related surgical complications.
🔬 Section 4 — The Differential Diagnosis Engine: Systematic Discrimination Mastery


⚖️ Section 5 - The Treatment Algorithm Matrix: Evidence-Based Intervention Mastery
Loading diagram…
📌 Remember: SURGICAL algorithm - Severity assessment, Underlying cause, Repair technique selection, Graft requirements, Incision planning, Closure method, Adjustment capability, Long-term outcomes. Each factor influences surgical success rates significantly.
- Ptosis Surgery Algorithm
- Aponeurotic Repair (Levator function >12mm)
- Success rate: >95% for 2-3mm ptosis
- Technique: Aponeurosis advancement 2-3mm per 1mm correction
- Complications: Overcorrection <5%, undercorrection 8-12%
- Frontalis Suspension (Levator function <8mm)
- Success rate: 85-90% with autogenous fascia lata
- Material selection: Fascia lata for <3 years old, silicone for adults
- Revision rate: 15-20% within 5 years
- Aponeurotic Repair (Levator function >12mm)
| Surgical Approach | Levator Function | Success Rate | Revision Rate | Complication Profile | Long-term Satisfaction |
|---|---|---|---|---|---|
| Aponeurosis Repair | >12mm | >95% | <10% | Minimal | >90% |
| Müller Resection | >12mm | 85-90% | 15% | Dry eye risk | 85% |
| Levator Resection | 8-12mm | 90-95% | 10-15% | Moderate | 88% |
| Frontalis Suspension | <8mm | 85-90% | 20% | Brow changes | 80% |
| Frontalis Sling | <4mm | 80-85% | 25% | Multiple procedures | 75% |
Ectropion Treatment Algorithm:
- Involutional Ectropion (Horizontal laxity >6mm)
- Lateral tarsal strip: Success rate >90% for mild-moderate cases
- Full-thickness wedge resection: 2-3mm excision per 1mm correction needed
- Indications: Horizontal laxity >8mm with good skin quality
- Complications: Notching <5%, overcorrection 8-10%
- Combined procedures: Canthal tightening plus skin grafting
- Success rate: 85-90% for severe cases
- Revision rate: 15-20% within 2 years
Loading diagram…
💡 Master This: The lateral canthal angle measurement predicts surgical success rates. Angles >75 degrees require canthal repositioning procedures with >95% success, while simple tightening procedures fail in >60% of cases with severe canthal malposition.
- Entropion Treatment Protocols
- Spastic Entropion: Botulinum toxin injection (2.5-5 units)
- Success rate: 80-85% for 3-6 months
- Injection sites: 3-4 points along lower lid orbicularis
- Involutional Entropion: Retractor reinsertion plus horizontal tightening
- Success rate: >90% with combined approach
- Failure rate: >50% with isolated procedures
- Cicatricial Entropion: Posterior lamella grafting
- Graft materials: Mucous membrane, hard palate, amniotic membrane
- Success rate: 75-85% depending on severity
- Spastic Entropion: Botulinum toxin injection (2.5-5 units)
| Treatment Modality | Indication | Success Rate | Duration | Complications | Cost-Effectiveness |
|---|---|---|---|---|---|
| Botulinum Toxin | Spastic type | 80-85% | 3-6 months | Temporary weakness | High for temporary |
| Retractor Repair | Involutional | >90% | Permanent | Overcorrection 5% | Excellent |
| Mucous Membrane Graft | Cicatricial | 75-85% | Permanent | Graft failure 15% | Good for severe |
| Hard Palate Graft | Severe cicatricial | 85-90% | Permanent | Donor site morbidity | Moderate |
| Amniotic Membrane | Mild cicatricial | 70-80% | Permanent | Limited availability | Variable |
⚖️ Section 5 — The Treatment Algorithm Matrix: Evidence-Based Intervention Mastery


🔗 Section 6 - The Integration Nexus: Multi-System Mastery Architecture
📌 Remember: INTEGRATE systems - Innervation networks, Neurovascular supply, Tear film dynamics, Extraocular muscles, Glandular function, Reflex pathways, Aesthetic balance, Tissue healing, Eye protection mechanisms. Each system influences others through measurable pathways.
- Tear Film-Lid Position Integration
- Lid malposition effects: 1mm ectropion reduces tear film stability by 40%
- Blink dynamics: Incomplete closure increases evaporation rate 300-500%
- Normal blink rate: 15-20 per minute
- Incomplete blinks: >50% in computer users
- Tear film breakup: <10 seconds indicates instability
- Meibomian gland function: 25% gland loss per decade after age 40
- Gland dropout: Correlates with lid margin irregularities
- Oil layer thickness: 50-100nm for stability
- Dysfunction prevalence: >60% in patients >40 years
Loading diagram…
| System Integration | Normal Function | Mild Dysfunction | Severe Dysfunction | Cascade Effects | Intervention Threshold |
|---|---|---|---|---|---|
| Tear Film Stability | >15 seconds | 10-15 seconds | <10 seconds | Corneal damage | <10 seconds |
| Blink Completeness | 100% closure | 90-95% closure | <90% closure | Exposure keratopathy | <95% closure |
| Meibomian Function | >75% glands | 50-75% glands | <50% glands | Evaporative dry eye | <75% glands |
| Lid-Globe Apposition | Perfect contact | Minimal gap | >2mm gap | Tear pooling | >1mm gap |
| Neural Coordination | Synchronized | Slight delay | Dyscoordination | Functional failure | >100ms delay |
Facial Nerve-Oculoplastic Integration:
- Neural Pathway Complexity
- Facial nerve branches: Temporal and zygomatic provide dual innervation
- Cross-innervation patterns: 60-70% overlap between branches
- Recovery potential: Partial function in 85% of incomplete palsies
- Synkinesis development: 40-60% of recovered cases
- Sympathetic integration: Müller's muscle coordination with levator function
- Horner's syndrome: 1-2mm ptosis with normal levator function
- Compensatory mechanisms: Frontalis overaction in >90% of cases
💡 Master This: Synkinetic movements develop in 40-60% of facial nerve recovery cases, creating aberrant connections between eyelid closure and smile muscles. Understanding these patterns enables targeted botulinum toxin therapy with >85% improvement in functional outcomes.
-
Aesthetic-Functional Balance Integration
- Golden ratio proportions: Upper:middle:lower face ratio 1:1:0.8
- Palpebral fissure symmetry: <1mm difference acceptable
- Horizontal measurements: 28-30mm palpebral fissure width
- Vertical measurements: 9-12mm palpebral fissure height
- Canthal angle relationships: Medial and lateral canthi alignment
- Lateral canthal position: 2-4mm above medial canthal level
- Intercanthal distance: 30-35mm in adults
- Canthal tilt: 5-10 degrees upward slope optimal
-
Aging Integration Patterns
- Tissue elasticity loss: 20-30% reduction per decade
- Volume loss effects: Orbital fat atrophy creates apparent ptosis
- Fat pad herniation: Pseudoptosis from brow descent
- Skin redundancy: Mechanical ptosis from dermatochalasis
- Coordinated intervention: Multi-level approach for optimal outcomes
- Success rates: >90% with comprehensive planning
- Revision rates: <10% with integrated approach
Understanding these integration patterns enables comprehensive treatment planning that addresses root causes rather than isolated symptoms, achieving superior long-term outcomes with reduced revision rates.
🔗 Section 6 — The Integration Nexus: Multi-System Mastery Architecture


🎯 Section 7 - The Clinical Mastery Arsenal: Rapid Excellence Framework
Loading diagram…
📌 Remember: MASTERY framework - Measurement precision, Algorithm application, System integration, Timing optimization, Evidence utilization, Risk stratification, Yield maximization. Each component contributes to predictable excellence in clinical outcomes.
- Rapid Assessment Protocol (<3 minutes)
- Primary measurements: MRD1, levator function, lid laxity
- Secondary assessments: Symmetry, dynamics, associated signs
- Measurement accuracy: ±0.5mm for reliable decision making
- Documentation standards: Photographic and quantitative records
- Differential ranking: Probability-weighted diagnosis list
- Primary diagnosis: >80% confidence level
- Alternative diagnoses: Ranked by likelihood and treatment implications
| Assessment Component | Time Allocation | Critical Measurements | Decision Points | Accuracy Threshold |
|---|---|---|---|---|
| Initial Inspection | 30 seconds | Symmetry, obvious abnormalities | Bilateral vs unilateral | Visual assessment |
| Quantitative Measurement | 90 seconds | MRD1, levator function, laxity | Surgical candidacy | ±0.5mm precision |
| Dynamic Testing | 60 seconds | Fatigue, ice test, forced duction | Etiology determination | >2mm change significant |
| Documentation | 30 seconds | Photography, measurements | Treatment planning | Standardized protocol |
| Decision Formulation | 30 seconds | Algorithm application | Treatment selection | >80% confidence |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | ||||
| flowchart TD |
Start["👤 Patient Intake
• Clinical presentation• Initial history"]
Assess["📋 Rapid Assessment
• Evaluate vitals• Physical exam"]
MeasureCheck{"🔬 Measurements?
• Data complete• Values recorded"}
AddTesting["🧪 Additional Testing
• Labs and imaging• Specific panels"]
Algo["⚙️ Algorithm
• Apply protocol• Process data"]
ConfCheck{"🎯 Confidence >80%?
• Check threshold• Validate result"}
SpecConsult["👨⚕️ Specialist
• Expert review• Consult opinion"]
Treatment["💊 Tx Planning
• Set interventions• Dosing schedule"]
Outcome["📈 Prediction
• Expected results• Recovery path"]
Counsel["🗣️ Counseling
• Patient education• Informed consent"]
Start --> Assess Assess --> MeasureCheck MeasureCheck -->|Yes| Algo MeasureCheck -->|No| AddTesting AddTesting --> Algo Algo --> ConfCheck ConfCheck -->|Yes| Treatment ConfCheck -->|No| SpecConsult SpecConsult --> Treatment Treatment --> Outcome Outcome --> Counsel
style Start fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style Assess fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style MeasureCheck fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style AddTesting fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C style Algo fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252 style ConfCheck fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style SpecConsult fill:#EEFAFF, stroke:#DAF3FF, stroke-width:1.5px, rx:12, ry:12, color:#0369A1 style Treatment fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style Outcome fill:#F6F5F5, stroke:#E7E6E6, stroke-width:1.5px, rx:12, ry:12, color:#525252 style Counsel fill:#EEFAFF, stroke:#DAF3FF, stroke-width:1.5px, rx:12, ry:12, color:#0369A1
> ⭐ **Clinical Pearl**: The **"Rule of 15s"** provides rapid surgical planning: **15mm** levator function suggests **aponeurotic repair**, **15 units** botulinum toxin for **spastic entropion**, **15%** overcorrection target for **ptosis surgery**. This framework achieves **>90% appropriate** initial treatment selection.
**Evidence-Based Decision Matrix**:
* **Success Rate Predictions**
- **Aponeurotic ptosis repair**: **>95%** success with **>12mm** levator function
- **Frontalis suspension**: **85-90%** success with **<8mm** levator function
+ Material selection: **Autogenous fascia** for **children <3 years**
+ Synthetic materials: **Adults** with **limited donor sites**
- **Ectropion repair**: **>90%** success with **appropriate technique selection**
+ Lateral tarsal strip: **Mild-moderate** horizontal laxity
+ Wedge resection: **Severe laxity** with **good skin quality**
| Clinical Scenario | First-Line Treatment | Success Rate | Alternative Options | Revision Rate | Patient Satisfaction |
|-------------------|---------------------|--------------|-------------------|---------------|---------------------|
| Mild Aponeurotic Ptosis | Aponeurosis repair | **>95%** | Müller resection | **<5%** | **>95%** |
| Severe Congenital Ptosis | Frontalis suspension | **85-90%** | Levator resection | **15-20%** | **80-85%** |
| Involutional Ectropion | Lateral tarsal strip | **>90%** | Wedge resection | **<10%** | **>90%** |
| Cicatricial Entropion | Posterior graft | **75-85%** | Anterior approach | **20-25%** | **75-80%** |
| Facial Nerve Palsy | Gold weight | **>85%** | Tarsorrhaphy | **10-15%** | **80-85%** |> 💡 **Master This**: **Complication prediction models** enable **proactive management**. Patients with **>3 risk factors** (age >70, diabetes, previous surgery, poor tissue quality, unrealistic expectations) have **>40% complication rates**, requiring **modified surgical approaches** and **enhanced counseling protocols**.
* **Quality Metrics Dashboard**
- **Surgical outcomes**: **Success rate >90%**, **revision rate <15%**
- **Patient satisfaction**: **>85%** excellent ratings
+ Functional improvement: **Objective measurement** improvement
+ Aesthetic satisfaction: **Standardized questionnaire** scores
- **Complication rates**: **<10%** significant complications
+ Minor complications: **Temporary swelling**, **bruising**
+ Major complications: **Overcorrection**, **undercorrection**, **infection**
* **Continuous Improvement Framework**
- **Outcome tracking**: **Systematic data collection** for **>500 cases**
- **Pattern recognition**: **Complication analysis** and **prevention strategies**
- **Technique refinement**: **Evidence-based modifications** for **improved outcomes**
+ Learning curve: **50-100 cases** for **technique mastery**
+ Outcome optimization: **Continuous refinement** based on **data analysis**
This mastery framework enables **consistent excellence** through **systematic application** of **evidence-based principles**, achieving **predictable outcomes** that exceed **patient expectations** while **minimizing complications** and **revision procedures**.
🎯 Section 7 — The Clinical Mastery Arsenal: Rapid Excellence Framework
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more












Have doubts about this lesson?
Ask Rezzy, your AI Study Partner, to explain anything you didn't understand
Everything you need for NEET-PG prep
Get full Oncourse access with lessons, practice questions, flashcards and AI study tools.
Scan to download app