

Introduction & Tear Film - Tear Trouble
- Dry Eye Disease (DED): Multifactorial; loss of tear film homeostasis, symptoms of discomfort, visual disturbance, tear film instability, potential ocular surface damage.
- Tear Film (3 layers):
- Lipid (Outer): Meibomian glands; prevents evaporation, maintains surface tension.
- Aqueous (Middle): Lacrimal glands; oxygen, nutrients, antimicrobials.
- Mucin (Inner): Goblet cells; corneal wettability, adherence.

⭐ Tear Film Break-Up Time (TBUT) < 10s is a key indicator of evaporative dry eye disease (EDED).
Etiopathogenesis - Why So Dry?
- Core Problem: Tear film instability → hyperosmolarity, inflammation, surface damage.
- Two Main Pathways:
- Aqueous Deficient (ADDE): ↓ tear production.
- Sjögren's: Autoimmune; lacrimal/salivary glands.
- Non-Sjögren's: Lacrimal dysfunction (age, inflammation, drugs e.g., antihistamines, β-blockers).
- Evaporative (EDE): ↑ tear evaporation.
- Intrinsic: Meibomian Gland Dysfunction (MGD) - most common DED cause.
- Extrinsic: Vit A deficiency, preservatives (BAK), contact lenses, low blink.
- Aqueous Deficient (ADDE): ↓ tear production.
- The Vicious Cycle of DED:
Loading diagram…
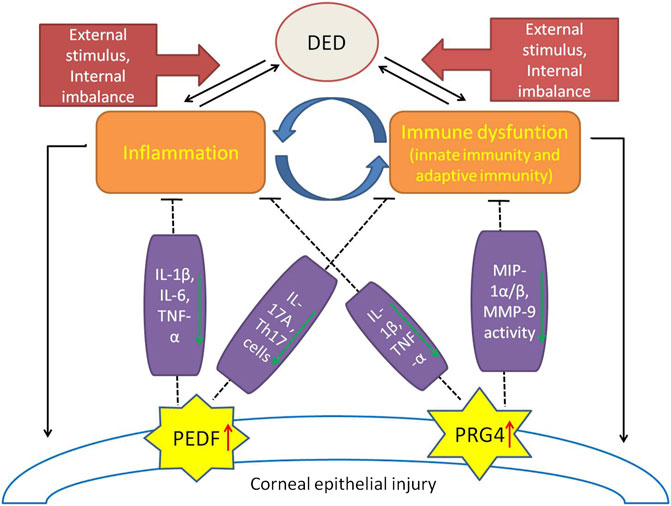
⭐ Inflammation (cytokines like IL-1, MMP-9) is a key driver in DED's vicious cycle, common to both ADDE & EDE.
Classification & Clinical Features - Dryness Decoded
- Two Main Categories (DEWS II):
- Aqueous Deficient (ADDE):
- Sjögren Syndrome (SSDE): Autoimmune.
- Non-Sjögren (NSSDE): Lacrimal damage, ↓reflex secretion.
- Evaporative (EDE):
- Intrinsic: Meibomian Gland Dysfunction (MGD), poor lid apposition.
- Extrinsic: Vitamin A deficiency, preservatives, contact lens.
- Aqueous Deficient (ADDE):
- Symptoms: Dryness, grittiness, burning, photophobia, fluctuating vision.
- Signs:
- ↓ Tear Break-Up Time (TBUT) < 10s.
- Corneal/conjunctival staining (fluorescein, lissamine green).
- ↓ Schirmer test (e.g., < 5mm/5min in SSDE).
- Lid margin changes (MGD signs).
⭐ Meibomian Gland Dysfunction (MGD) is the leading cause of Evaporative Dry Eye (EDE) worldwide.
Diagnostic Workup - Tear Test Time
- Schirmer's Test: Assesses tear production.
- Schirmer I (no anesthesia): Basal + Reflex. Normal: >15 mm/5min. DED: <10 mm (mild), <5 mm (severe).
- Schirmer II (anesthesia): Basal secretion.
- Tear Film Break-Up Time (TBUT): Evaluates tear film stability.
- Fluorescein instilled. Normal: >10 sec. DED: <10 sec.
⭐ TBUT <5 sec strongly indicates severe DED & tear instability.
- Ocular Surface Staining:
- Fluorescein: Detects corneal epithelial defects.
- Lissamine Green / Rose Bengal: Stains devitalized cells.
- Advanced: Tear osmolarity (>308 mOsm/L), MMP-9 levels.
Loading diagram…
Management Strategies - Moisture Mission
- Goal: Restore homeostasis, improve tear stability, reduce symptoms.
- Stepwise Approach:
- Level 1:
- Education, environmental mods.
- Artificial tears (ATs): Preservative-free (PF) if >4 uses/day. Lipid-based for MGD.
- Lid hygiene (MGD).
- Level 2 (if inadequate):
- Punctal occlusion.
- Topical anti-inflammatories:
- Corticosteroids (Loteprednol): short-term. ⚠️ IOP.
- Cyclosporine A (0.05%), Lifitegrast: long-term. 📌 (CALI: Cyclo & Lifi)
- Level 3 (severe DED):
- Autologous Serum Eye Drops (ASEDs).
- Oral secretagogues (Pilocarpine).
- Therapeutic contact lenses.
- Level 1:
⭐ Cyclosporine A (0.05%) increases tear production by inhibiting T-cell activation; may take 3-6 months for full effect.
Loading diagram…
High‑Yield Points - ⚡ Biggest Takeaways
- Dry Eye Disease (DED): Multifactorial ocular surface disease from tear film instability.
- Types: Aqueous Deficient (e.g., Sjögren's) & Evaporative (most common, e.g., MGD).
- Symptoms: Burning, grittiness, foreign body sensation, fluctuating vision.
- Key tests: TBUT < 10s, Schirmer's < 10mm/5min, corneal staining.
- Meibomian Gland Dysfunction (MGD) is the most common cause of DED.
- Management: Artificial tears, cyclosporine A, lifitegrast, punctal plugs, lid hygiene.
- Sjögren's syndrome: Severe DED; associated with anti-Ro/SSA & anti-La/SSB antibodies.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more