

Overview & Principles - Setting the Stage
- Context: Addresses gender incongruence, aiming to align an individual's physical characteristics with their affirmed gender identity.
- Guiding Framework: World Professional Association for Transgender Health (WPATH) Standards of Care, currently SOC 8.
- Core Tenets:
- Thorough assessment: medical, mental health, social context.
- Informed consent: comprehensive, covering risks, benefits, alternatives, and irreversibility of surgical procedures.
- Multidisciplinary Team (MDT) approach is crucial for holistic care.
Loading diagram…
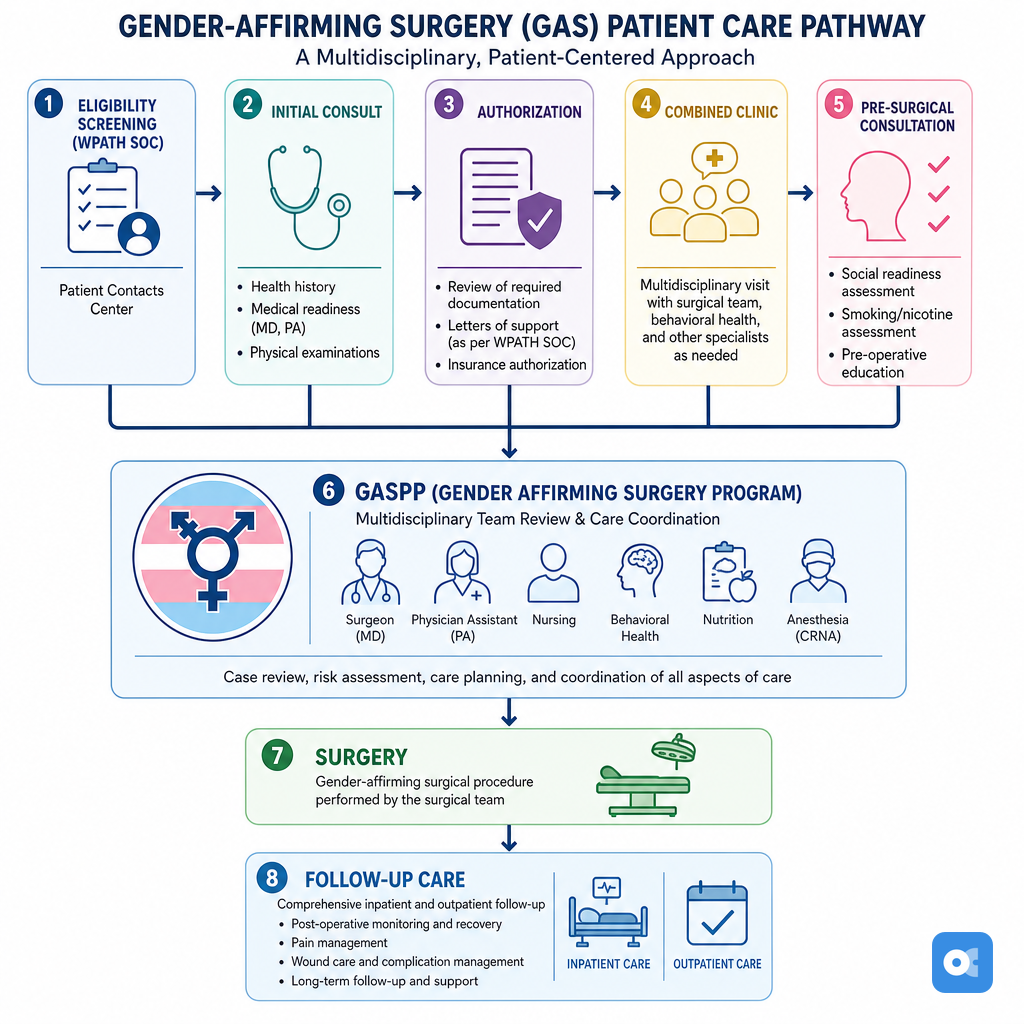
⭐ As per WPATH SOC, eligibility for many gender-affirming surgeries requires documentation of persistent gender incongruence and capacity to consent; often includes a period of hormone therapy and real-life experience (RLE).
Feminizing Procedures - Crafting Congruence
Aligns physical characteristics with female gender identity. Multidisciplinary team approach is key.
- Vaginoplasty: Primary genital surgery; creates neovagina, clitoris, labia.
- Techniques: Penile Inversion (PIV) - most common; Intestinal (sigmoid); Peritoneal Pull-Through.
- Aims: Aesthetic, functional (coitus, sensation) outcomes.
- Orchiectomy: Bilateral testicular removal.
- Significantly ↓ testosterone; reduces anti-androgen need.
- Standalone or pre-vaginoplasty.
- Breast Augmentation: Enhances breast volume/contour.
- Methods: Implants (silicone/saline), autologous fat transfer.
- Facial Feminization Surgery (FFS): Suite of procedures to feminize facial features.
- Common: Forehead contouring, rhinoplasty, genioplasty, jaw reduction, hairline advancement.
- Voice Feminization Surgery: Raises vocal pitch.
- Techniques: Cricothyroid approximation (CTA), thyroplasty.
- Tracheal Shave (Chondrolaryngoplasty): Reduces thyroid cartilage prominence (Adam's apple).
Loading diagram…

⭐ Penile inversion vaginoplasty (PIV) is the most commonly performed technique for neovagina creation, utilizing penile and scrotal skin for the neovaginal lining and labia minora construction respectively, offering good aesthetic and functional results including tactile sensation.
Masculinizing Procedures - Building Authenticity
Aligns physical traits with male gender identity.
- Chest (Top Surgery):
- Mastectomy: Techniques (e.g., double incision, periareolar) vary by breast size/elasticity.
- Goal: Male chest contour, nipple/areola reconstruction.
- Genital (Bottom Surgery):
- Hysterectomy +/- Bilateral Salpingo-oophorectomy (BSO): Removes uterus/ovaries.
- Phalloplasty: Neophallus creation (e.g., Radial Forearm Free Flap (RFFF), Anterolateral Thigh (ALT) flaps). Multi-stage. Urethroplasty for standing voiding.
- Metoidioplasty: Clitoral release (post-testosterone). Simpler, smaller neophallus.
- Scrotoplasty: Creates scrotum; testicular implants.
- Vaginectomy: Vaginal removal/closure.
- Other: Facial masculinization surgery (FMS); voice surgery (e.g., thyroplasty) less common due to testosterone effects.
⭐ Phalloplasty offers a larger neophallus and standing micturition but is multi-stage with higher complication rates (e.g., urethral strictures, fistulas) than metoidioplasty.
Loading diagram…
Complications & Follow-up - Navigating Recovery
- General Risks: Infection, bleeding, DVT/PE, pain, adverse scarring.
- Procedure-Specific:
- Vaginoplasty: Neovaginal stenosis (requires dilation), fistula, prolapse.
- Phalloplasty: Urethral stricture/fistula, flap compromise, implant issues.
- Mastectomy: Hematoma, seroma, contour irregularities.
- Long-term Care: Regular check-ups, hormone management, psychological support, lifelong surveillance.
- Revisional Surgery: May be needed for functional or aesthetic concerns.
Loading diagram…
⭐ Post-vaginoplasty, lifelong adherence to a dilation schedule is critical to prevent neovaginal stenosis.
High‑Yield Points - ⚡ Biggest Takeaways
- Masculinizing surgeries: phalloplasty/metoidioplasty, scrotoplasty, testicular implants.
- Feminizing surgeries: vaginoplasty (penile inversion common), labiaplasty, clitoroplasty.
- Chest masculinization (subcutaneous mastectomy) is often the first/only surgery for transmasculine individuals.
- Breast augmentation (mammoplasty) is common for transfeminine individuals.
- Hysterectomy/oophorectomy in transmasculine individuals aids hormonal stability, reduces cancer risk.
- Orchiectomy in transfeminine individuals primarily for testosterone suppression, gonad removal.
- Facial surgery (FFS/FMS) and voice surgery are adjunctive options for congruence.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more