

Dialysis Access - Kidney's Best Friend
- Lifeline for End-Stage Renal Disease (ESRD) patients needing Hemodialysis (HD).
- Provides reliable, long-term vascular access for efficient blood purification.
- Indications for HD initiation & access planning:
- GFR < 15 mL/min/1.73m² (CKD Stage 5)
- Symptomatic uremia (e.g., pericarditis, encephalopathy)
- Refractory hyperkalemia, fluid overload, or acidosis
⭐ Plan for access creation when GFR < 20-25 mL/min or 6-12 months before anticipated HD start to allow maturation.
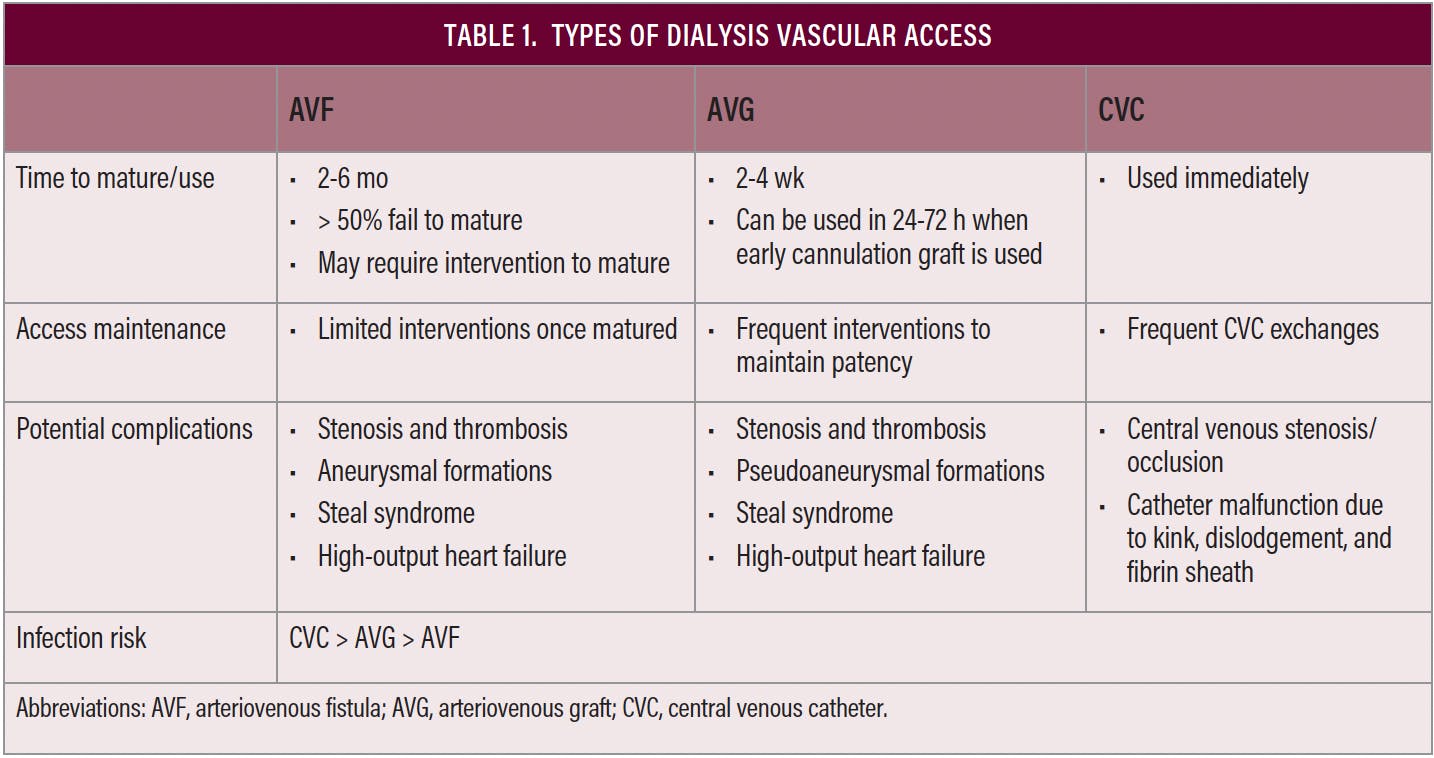
Access Types - Vein, Graft, or Catheter?
- KDOQI Preference: AVF > AVG > CVC (Fistula First)
- 1. Arteriovenous Fistula (AVF) - Gold Standard
- Anastomosis: Native artery to vein (e.g., Radiocephalic).
- Pros: Best patency, ↓complications (infection, thrombosis).
- Cons: Maturation 6-12 weeks (or longer); primary failure common.
⭐ Rule of 6s (mature AVF): Flow >600mL/min, Diameter >6mm, Depth <6mm, Length >6cm.
- 2. Arteriovenous Graft (AVG)
- Material: Synthetic tube (PTFE) bridging artery & vein.
- Pros: Usable 2-4 weeks; for poor veins.
- Cons: ↑Stenosis (venous anastomosis), thrombosis, infection vs AVF.
- 3. Central Venous Catheter (CVC)
- Types: Tunneled (long-term), Non-tunneled (short-term/urgent).
- Pros: Immediate use; bridge access.
- Cons: Highest risk: infection (BSI), central vein stenosis.
- Site: RIJV preferred; avoid subclavian (stenosis).

Pre-Op Planning - Measure Twice, Cut Once
- Clinical Evaluation:
- History: Prior access, central lines, pacemakers, IVDU, dominant arm.
- Exam: Bilateral BP, pulses, Allen's Test (crucial for radiocephalic AVF), vein inspection & palpation (with tourniquet).
- Duplex Ultrasound (Vessel Mapping): Essential for optimal site selection.
- Artery: Diameter ≥2mm, patent, pliable, no significant stenosis or heavy calcification.
- Vein: Diameter ≥2.5mm (AVF), ≥4mm (AVG); patent, compressible, continuous with central veins, depth <0.6cm.
⭐ Pre-operative duplex ultrasound vessel mapping is crucial; it significantly improves primary AVF patency rates.
- Pre-Op Decision Flow:
Loading diagram…
Creation to Complications - The Access Journey
- Access Creation:
- AVF (Arteriovenous Fistula): Gold standard; direct artery-vein anastomosis.
- Preferred sites (distal first): Radio-cephalic (Brescia-Cimino), Brachio-cephalic, Brachio-basilic (transposed).
- AVG (Arteriovenous Graft): Synthetic (PTFE) conduit if native veins unsuitable. Higher thrombosis & infection rates.
- AVF (Arteriovenous Fistula): Gold standard; direct artery-vein anastomosis.
- Maturation & "Rule of 6s" (📌) (AVF: 4-8 weeks, ideally ~6):
- Blood Flow: > 600 mL/min.
- Diameter (vein): > 6 mm.
- Depth from skin: < 6 mm (for easy cannulation).
- Cannulatable segment length: > 6 cm.
- Monitoring:
- Clinical Exam: Palpable thrill, audible bruit (continuous).
- Duplex Ultrasound: Confirms maturation, measures flow, detects stenosis/patency.
- Complications & Management:
Loading diagram…
* **Thrombosis**: Most common failure. Rx: Thrombectomy (surgical/mechanical), thrombolysis.
* **Stenosis**: Typically venous outflow.
> ⭐ Juxta-anastomotic venous stenosis is the most common site of stenosis in AVFs.
* Rx: PTA (angioplasty) ± stenting.
* **Infection**: ↑ in AVGs. Local signs (erythema, pus) + systemic (fever). Rx: Antibiotics; graft excision if severe/persistent.
* **Steal Syndrome**: Distal arterial hypoperfusion. Symptoms: Pain, pallor, paresthesia, ↓pulses. Rx: Banding, DRIL procedure.
* **Aneurysm/Pseudoaneurysm**: From repeated cannulation/wall weakness. Rx: Surgical repair if symptomatic, large, skin changes, or risk of rupture.
* **High-Output Cardiac Failure**: Rare; with large, high-flow proximal AVFs.
High‑Yield Points - ⚡ Biggest Takeaways
- Radiocephalic AVF (Brescia-Cimino) is the preferred initial hemodialysis access.
- Rule of 6s for AVF maturity: 6mm diameter, <6mm depth, >600mL/min flow, 6 weeks to use.
- PTFE grafts: use if veins unsuitable; higher infection and thrombosis risk.
- Central venous catheters: for temporary/urgent access; highest infection risk.
- Common complications: stenosis, thrombosis, infection, steal syndrome, aneurysm.
- Palpable thrill and audible bruit indicate AVF patency.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more