

H&N Cancer Overview - Basics & Bad Habits
- Predominantly Squamous Cell Carcinomas (SCC) >90% from upper aerodigestive tract (UADT) mucosa.
- India: High incidence, often linked to regional habits like tobacco and betel quid chewing.
- Key Risk Factors ("Bad Habits"):
- Tobacco (smoking/smokeless): Primary etiological agent, dose-response relationship. 📌 Tobacco: Chief Culprit.
- Alcohol: Synergistic effect with tobacco, significantly ↑ risk.
- Betel Quid (Areca nut): Strong association with oral cancer; causes Oral Submucous Fibrosis (OSMF) - a precancerous condition.
- Human Papillomavirus (HPV): Mainly HPV-16, linked to oropharyngeal cancers (tonsil, base of tongue); generally better prognosis.
- Others: Poor oral hygiene, chronic irritation, radiation exposure, nutritional deficiencies (e.g., Plummer-Vinson syndrome).
⭐ Over 75% of head and neck cancers are linked to tobacco use (smoked or smokeless).

Staging & Spread - Mapping the Mayhem
-
TNM System (AJCC 8th Ed. principles):
- T (Tumor): Size & local invasion (T1-T4).
- N (Nodes): Regional lymph node status (N0-N3).
- N0: No nodes.
- N1: Single ipsilateral, ≤ 3cm.
- N2: Ipsilateral > 3cm-6cm / Multiple ipsi / Bilateral/Contralateral (all ≤ 6cm).
- N3: Node > 6cm / Any node with Extranodal Extension (ENE).
- M (Metastasis): M0 (no distant), M1 (distant).
-
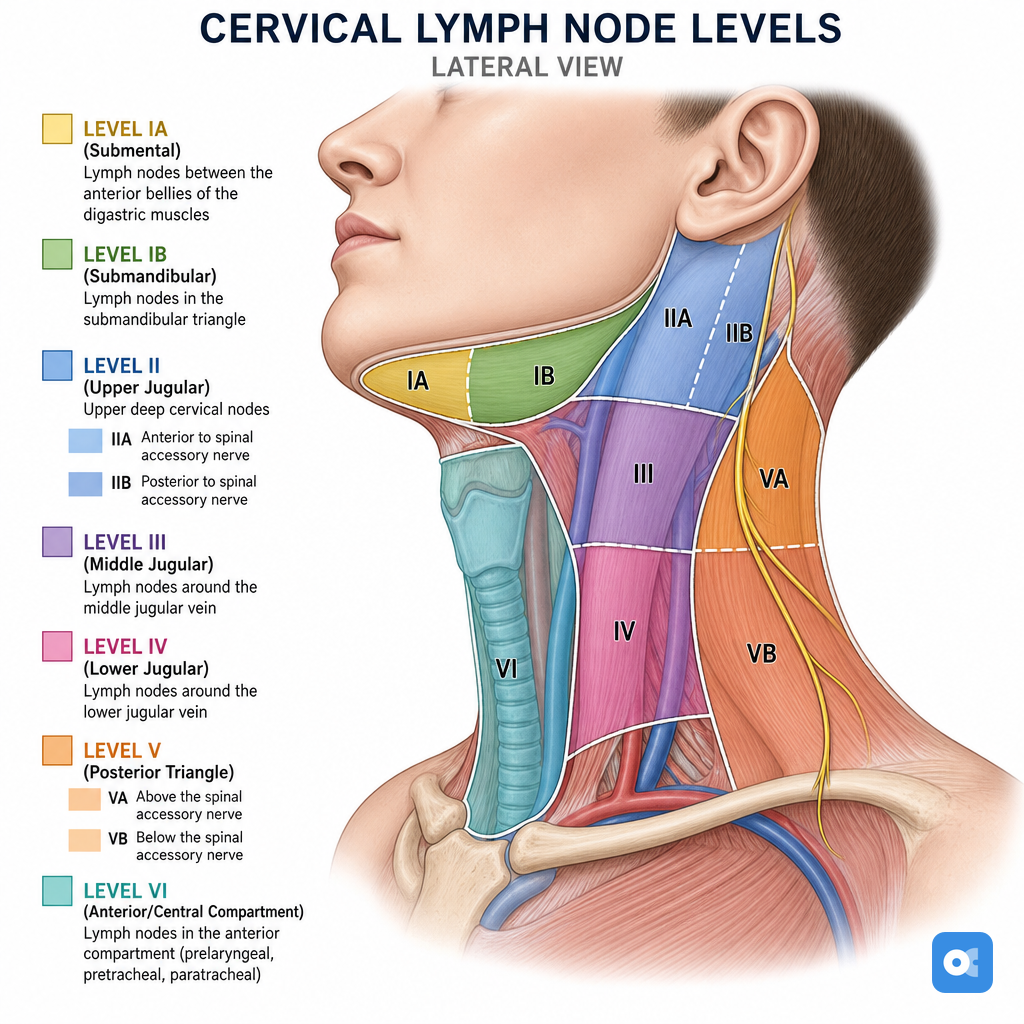
Key Neck Nodal Levels:
- I: Submental/Submandibular
- II: Upper Jugular
- III: Middle Jugular
- IV: Lower Jugular
- V: Posterior Triangle
- VI: Anterior Compartment
-
Spread Patterns:
- Lymphatic: Common, predictable.
- Hematogenous: Lungs, liver, bone.
⭐ Extracapsular spread (ECS) or Extranodal Extension (ENE) in lymph nodes (pN+) significantly worsens prognosis and often indicates need for adjuvant chemoradiotherapy.
Clinical Clues & Diagnosis - Signs & Sleuthing
- Key Symptoms (Red Flags):
- Oral: Non-healing ulcer/patch (>3 wks), pain, bleeding, trismus, loose teeth.
- Laryngeal: Persistent hoarseness (>3 wks), stridor, dysphagia, hemoptysis.
- Pharyngeal: Sore throat, dysphagia, odynophagia, referred otalgia (Trotter's - NPC), globus.
- Nasal/Sinus: Unilateral obstruction, epistaxis, facial swelling/pain, proptosis.
- Neck: Persistent lump (often painless, firm, fixed, >2cm).
- General: Unexplained weight loss, fatigue.
- Diagnostic Approach:
Loading diagram…
> ⭐ Histopathological confirmation via biopsy is mandatory. FNAC is the primary step for suspicious neck nodes.
* **Imaging:** CT (bone, nodes), MRI (soft tissue, perineural spread), PET-CT (mets, unknown primary).
Management Modalities - Treatment Takedown
- Goal: Maximize cure, preserve organ function & Quality of Life (QoL). Multidisciplinary Team (MDT) essential.
- Core Modalities:
- Surgery: Primary for most resectable tumors (oral cavity, larynx, salivary). Includes neck dissection (therapeutic/prophylactic). Reconstruction often needed (e.g., PMMC, free flaps).
- Radiotherapy (RT): Definitive (e.g., early larynx, NPC), adjuvant (post-op), or palliative. Techniques: EBRT (IMRT, VMAT), Brachytherapy. Key toxicities: mucositis, xerostomia.
- Chemotherapy (CT): Used as induction, concurrent with RT (CRT - a standard), adjuvant, or palliative. Agents: Cisplatin, 5-FU, Taxanes. Targeted therapy: Cetuximab (EGFR inhibitor).
- Immunotherapy: PD-1 inhibitors (Nivolumab, Pembrolizumab) for recurrent/metastatic settings.
- Treatment Choice: Depends on primary site, TNM stage, histology, patient's performance status, and comorbidities.
⭐ Concurrent chemoradiation (CRT) with high-dose Cisplatin (100 mg/m²) is a standard backbone for locally advanced SCCHN, offering improved locoregional control and survival over RT alone for many sites.
High‑Yield Points - ⚡ Biggest Takeaways
- Squamous Cell Carcinoma (SCC) is the most common head and neck cancer, strongly linked to tobacco and alcohol.
- HPV infection, particularly HPV-16, is a key risk factor for oropharyngeal cancers.
- Nasopharyngeal carcinoma is associated with EBV infection and often presents with neck nodes.
- Leukoplakia and erythroplakia are critical oral premalignant lesions requiring biopsy.
- Neck node metastasis is the single most important prognostic factor in H&N SCC.
- FNAC is the initial investigation of choice for most palpable neck masses.
- Early-stage disease often involves single-modality treatment; advanced stages typically require multimodality approaches.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more